You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
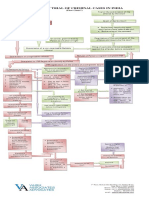
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- ADUtilitiesDocument4 pagesADUtilitiesapi-3745837No ratings yet
- Investment ChecklistDocument3 pagesInvestment ChecklistArpan chakrabortyNo ratings yet
- MinimumEHS Standards For Projects-V3Document113 pagesMinimumEHS Standards For Projects-V3Ammu KuttiyNo ratings yet
- BBC Focus - Answers To Lifes Big Questions 2017Document100 pagesBBC Focus - Answers To Lifes Big Questions 2017AD StrategoNo ratings yet
- PETITION For Declaration of NullityDocument7 pagesPETITION For Declaration of NullityKira Jorgio100% (3)
- Features of Contingency Approach To ManagementDocument9 pagesFeatures of Contingency Approach To ManagementSharon AmondiNo ratings yet
- EScholarship UC Item 8k05n5csDocument10 pagesEScholarship UC Item 8k05n5csAnonymous pJfAvlNo ratings yet
- Aafp PDFDocument8 pagesAafp PDFAnonymous umFOIQIMBANo ratings yet
- Left Ovarian Brenner Tumor: Key-Word: Ovary, NeoplasmsDocument2 pagesLeft Ovarian Brenner Tumor: Key-Word: Ovary, NeoplasmsAnonymous pJfAvlNo ratings yet
- Executive Summary of Methanol Poisoning - 03Document13 pagesExecutive Summary of Methanol Poisoning - 03Anonymous pJfAvl100% (1)
- Oxygen-Free Radicals Impair Fracture Healing in Rats: A Were ofDocument3 pagesOxygen-Free Radicals Impair Fracture Healing in Rats: A Were ofAnonymous pJfAvlNo ratings yet
- Juzaili Alias SSB Jadual Perubahan PDP Dan Penilaian AlternatifDocument1 pageJuzaili Alias SSB Jadual Perubahan PDP Dan Penilaian Alternatifkar afiNo ratings yet
- Swift Case Study Mapping A Path To Iso 20022 With Swift Translator Jan2022Document3 pagesSwift Case Study Mapping A Path To Iso 20022 With Swift Translator Jan2022Bolaji EsanNo ratings yet
- Programming Essentials in PythonDocument23 pagesProgramming Essentials in PythonNabeel AmjadNo ratings yet
- $RV3E842Document78 pages$RV3E842Dorian VoineaNo ratings yet
- Unit Test 9 BDocument1 pageUnit Test 9 BAnnaNo ratings yet
- MVP Teacher 12Document6 pagesMVP Teacher 12Ivan ChuNo ratings yet
- Policy ScheduleDocument1 pagePolicy ScheduleDinesh nawaleNo ratings yet
- Climate Change Forests and Forest Management An O-Wageningen University and Research 481068Document145 pagesClimate Change Forests and Forest Management An O-Wageningen University and Research 481068gulnuromar034No ratings yet
- Ingles V Eje 1 Week 2Document5 pagesIngles V Eje 1 Week 2Cristhian Javier Torres PenaNo ratings yet
- Microwave Oven: Instructions & Cooking GuideDocument38 pagesMicrowave Oven: Instructions & Cooking GuidethomaselandNo ratings yet
- Indian Board of Alternative Medicine: Partner-Pub-1166 ISO-8859-1Document14 pagesIndian Board of Alternative Medicine: Partner-Pub-1166 ISO-8859-1vipinNo ratings yet
- 7 Types of English Adjectives That Every ESL Student Must KnowDocument3 pages7 Types of English Adjectives That Every ESL Student Must KnowBenny James CloresNo ratings yet
- Introduction To Strategic Cost Management and Management AccountingDocument3 pagesIntroduction To Strategic Cost Management and Management AccountingnovyNo ratings yet
- Technical ReportDocument39 pagesTechnical ReportTope-Akanni AyomideNo ratings yet
- Physical Medicine Rehabilitation Brochure Bangkok 2020Document6 pagesPhysical Medicine Rehabilitation Brochure Bangkok 2020nur yulia sariNo ratings yet
- Finals Lesson Ii Technology As A WAY of Revealing: Submitted By: Teejay M. AndrdaDocument8 pagesFinals Lesson Ii Technology As A WAY of Revealing: Submitted By: Teejay M. AndrdaTeejay AndradaNo ratings yet
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Document3 pagesHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniNo ratings yet
- SHARE SEA Outlook Book 2518 r120719 2Document218 pagesSHARE SEA Outlook Book 2518 r120719 2Raafi SeiffNo ratings yet
- ORtHOGRAPHIC Plan FinalDocument8 pagesORtHOGRAPHIC Plan FinalKrizzie Jade CailingNo ratings yet
- Practical No 4Document5 pagesPractical No 4Mahin SarkarNo ratings yet
- 9701 w19 QP 21 PDFDocument12 pages9701 w19 QP 21 PDFFaiza KhalidNo ratings yet
- Analytical ReasoningDocument7 pagesAnalytical ReasoningKashif NadeemNo ratings yet
- Rhetorical Analysis EssayDocument8 pagesRhetorical Analysis Essayapi-308821140No ratings yet