You might also like
- From Acute To Chronic Back PainDocument607 pagesFrom Acute To Chronic Back PainHugo Falqueto100% (2)
- Hamstring Strain Injuries JOSPTDocument18 pagesHamstring Strain Injuries JOSPTHugo FalquetoNo ratings yet
- NP Outreach Curriculum in Rheumatology St. Joseph's Health Care, London, ON Dr. Sherry Rohekar November 12, 2009Document50 pagesNP Outreach Curriculum in Rheumatology St. Joseph's Health Care, London, ON Dr. Sherry Rohekar November 12, 2009lynkx864100% (1)
- History of nursing development and rolesDocument29 pagesHistory of nursing development and rolesMitchee ZialcitaNo ratings yet
- Thoracic Outlet SyndromeDocument8 pagesThoracic Outlet SyndromeJong-soo KimNo ratings yet
- What Is Osteoporosis?: Osteoposis Is A Disease ofDocument48 pagesWhat Is Osteoporosis?: Osteoposis Is A Disease ofTaruna GargNo ratings yet
- OsteoarthritisDocument5 pagesOsteoarthritisRobby Dwitria MaulanaNo ratings yet
- Subacute Combined Degeneration of Spinal CordDocument4 pagesSubacute Combined Degeneration of Spinal CordPriyanka MathurNo ratings yet
- Overview Congenital Musculoskeletal DisorderDocument84 pagesOverview Congenital Musculoskeletal DisorderRyan Trian100% (3)
- Head Trauma Causes, Symptoms, Diagnosis and TreatmentDocument50 pagesHead Trauma Causes, Symptoms, Diagnosis and TreatmentNatasya Saraswati100% (1)
- By: Calaour, Carrey Dasco, Danica Amor Dimatulac, Kevin Lim, Shiela Marie Pagulayan, Sheena May Pua, Mar KristineDocument41 pagesBy: Calaour, Carrey Dasco, Danica Amor Dimatulac, Kevin Lim, Shiela Marie Pagulayan, Sheena May Pua, Mar Kristineceudmd3d100% (2)
- Back PainDocument35 pagesBack PainAugusto Moreno Quiropraxia100% (1)
- Pelvic Physical Therapy For Chronic Pain and Dysfunction FollowinDocument13 pagesPelvic Physical Therapy For Chronic Pain and Dysfunction Followincode PVSNo ratings yet
- Health, Stress, and CopingDocument43 pagesHealth, Stress, and CopingKar Gayee100% (1)
- Granulomatous Mastitis - A Case ReportDocument3 pagesGranulomatous Mastitis - A Case ReportqalbiNo ratings yet
- PATHOPHYSIOLOGY OF SHOCKDocument56 pagesPATHOPHYSIOLOGY OF SHOCKDr. Haricharan ANo ratings yet
- Hemodialysis Removes Wastes and Fluids From BloodDocument23 pagesHemodialysis Removes Wastes and Fluids From BloodAvinder MannNo ratings yet
- Clinical Reasoning For Nursing Students - Glossary of TermsDocument22 pagesClinical Reasoning For Nursing Students - Glossary of Termsmillstoneridge1100% (1)
- Causes, Types & Relief of HeadachesDocument7 pagesCauses, Types & Relief of HeadachesFiruzz TrojanersNo ratings yet
- Bon Ku - Ellen Lupton - Health Design Thinking - Creating Products and Services For Better HealthDocument226 pagesBon Ku - Ellen Lupton - Health Design Thinking - Creating Products and Services For Better HealthMilena Gomez100% (2)
- Spondylosis2 PDFDocument13 pagesSpondylosis2 PDFdrwarigitNo ratings yet
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocument96 pagesN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaNo ratings yet
- Primary Health Centre ReportDocument12 pagesPrimary Health Centre ReportAkshay H.100% (1)
- Causes and Management of Syncope in DentistryDocument27 pagesCauses and Management of Syncope in DentistrySelvarathi KandhaswamyNo ratings yet
- Ectopic Pregnancy Nursing Care PlansDocument27 pagesEctopic Pregnancy Nursing Care Plansviper7967880% (20)
- Immunity: Immunity Is The Balanced State ofDocument1 pageImmunity: Immunity Is The Balanced State ofCarolina GasperNo ratings yet
- Frozen ShoulderDocument1 pageFrozen ShouldersyndyeNo ratings yet
- Types of ExcerciseDocument13 pagesTypes of ExcerciseTefera LeteboNo ratings yet
- Endocrine Response Ni FinalDocument35 pagesEndocrine Response Ni FinalSaktriawan ArifNo ratings yet
- Lung Transplant PathwayDocument39 pagesLung Transplant PathwayMohana Preethi MNo ratings yet
- Measuring and Understanding Blood PressureDocument44 pagesMeasuring and Understanding Blood PressureFarwaNo ratings yet
- Diagnosis Treatment of Back Pain MedicationsDocument41 pagesDiagnosis Treatment of Back Pain Medicationsrabin1994No ratings yet
- Local AnaestheticsDocument26 pagesLocal Anaestheticsv_vijayakanth7656No ratings yet
- Adrenal Gland: by Mickey & BillyDocument23 pagesAdrenal Gland: by Mickey & BillyGhaidaa Sadeq100% (1)
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- Lesions of Upper Motor Neurons and Lower Motor NeuronsDocument9 pagesLesions of Upper Motor Neurons and Lower Motor NeuronsAdhitya Rama Jr.No ratings yet
- Abdominal Palpation 4.0Document9 pagesAbdominal Palpation 4.0dm pamNo ratings yet
- Frank-Starling LawDocument5 pagesFrank-Starling LawNTA UGC-NETNo ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentJaydee Dalay100% (2)
- Bronchiectasis Pa Tho Physiology, Presentation and ManagementDocument8 pagesBronchiectasis Pa Tho Physiology, Presentation and ManagementCristhian MellaNo ratings yet
- Gullaine-Barré SyndromeDocument13 pagesGullaine-Barré SyndromeOnieBoy CurayagNo ratings yet
- Hip FractureDocument4 pagesHip Fracturemariafub100% (1)
- Organophosphorus Poisoning PDFDocument5 pagesOrganophosphorus Poisoning PDFEliuth Zamora100% (1)
- Burn Injury PathophysiologyDocument1 pageBurn Injury PathophysiologyMonique Ann DanoyNo ratings yet
- JRA Types, Symptoms, TreatmentDocument21 pagesJRA Types, Symptoms, TreatmentFarry DoankNo ratings yet
- Cerebellar Stroke Causes, Symptoms & TreatmentDocument17 pagesCerebellar Stroke Causes, Symptoms & TreatmentAna CotomanNo ratings yet
- Muscular System DisordersDocument36 pagesMuscular System DisordersShawn Henry CepedaNo ratings yet
- Dr. Niranjan Murthy H L: Asst. Prof., Dept. of Physiology Sree Siddhartha Medical College & Hospital, TumkurDocument29 pagesDr. Niranjan Murthy H L: Asst. Prof., Dept. of Physiology Sree Siddhartha Medical College & Hospital, Tumkurnirilib100% (6)
- Diuretic Treatment in Heart FailureDocument12 pagesDiuretic Treatment in Heart FailureRoberto López Mata100% (1)
- Neuromuscular Disorders in Geriatric PatientsDocument16 pagesNeuromuscular Disorders in Geriatric PatientsAhmed NasrNo ratings yet
- Referred PainDocument3 pagesReferred PainaspalavistaNo ratings yet
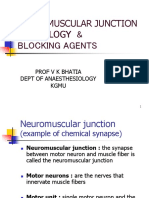
- Neuromuscular Junction Physiology & Blocking Agents: Prof V K Bhatia Dept of Anaesthesiology KgmuDocument39 pagesNeuromuscular Junction Physiology & Blocking Agents: Prof V K Bhatia Dept of Anaesthesiology KgmuAthira S MadhuNo ratings yet
- Introduction PhysiotherapistDocument12 pagesIntroduction Physiotherapistapi-371068989No ratings yet
- Anterior Cord SyndromeDocument8 pagesAnterior Cord SyndromeJanine Erika Julom BrillantesNo ratings yet
- The Circulatory System BookletDocument30 pagesThe Circulatory System BookletTroy CampbellNo ratings yet
- Fluid, Electrolyte, Acid Base BalanceDocument42 pagesFluid, Electrolyte, Acid Base BalanceSutrisno YangNo ratings yet
- New Techniques in Physical TherapyDocument61 pagesNew Techniques in Physical TherapyMohamed Magdy El MeligieNo ratings yet
- Understanding ALS: A Case Study of Mr. CooperDocument24 pagesUnderstanding ALS: A Case Study of Mr. CooperJeanessa Delantar QuilisadioNo ratings yet
- Juvenile Arthritis Symptoms, Causes, TreatmentsDocument8 pagesJuvenile Arthritis Symptoms, Causes, TreatmentsDhanNie CenitaNo ratings yet
- Evaluation and Management of Elevated Intracranial Pressure in AdultsDocument28 pagesEvaluation and Management of Elevated Intracranial Pressure in AdultssandykumalaNo ratings yet
- Acute Pain: Mechanisms, Management, and Treatment OptionsDocument61 pagesAcute Pain: Mechanisms, Management, and Treatment OptionsAnnisa RamadhanyNo ratings yet
- Lung SurgeriesDocument43 pagesLung SurgeriesSereinNo ratings yet
- GoitreDocument6 pagesGoitreJohn Vladimir A. BulagsayNo ratings yet
- Deglutition Reflex - LectureDocument38 pagesDeglutition Reflex - LectureasaadsarfrazNo ratings yet
- Turf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTurf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Beta Amiloid SleepDocument6 pagesBeta Amiloid SleepHugo FalquetoNo ratings yet
- Opioid and Chemokine Receptor - Nature (2015)Document10 pagesOpioid and Chemokine Receptor - Nature (2015)Hugo FalquetoNo ratings yet
- More Pain Less Gain ScienceDocument3 pagesMore Pain Less Gain ScienceHugo FalquetoNo ratings yet
- Repeated and Interrupted Resistance Exercise Induces The Desensitization and Re-Sensitization of mTOR-Related Signaling in Human Skeletal Muscle FibersDocument18 pagesRepeated and Interrupted Resistance Exercise Induces The Desensitization and Re-Sensitization of mTOR-Related Signaling in Human Skeletal Muscle FibersHugo FalquetoNo ratings yet
- Chronic Pain The Role of Learning and Brain Mansour-Farmer-Baliki-Apkarian - IB-04.01.2013Document31 pagesChronic Pain The Role of Learning and Brain Mansour-Farmer-Baliki-Apkarian - IB-04.01.2013Hugo FalquetoNo ratings yet
- A Systematic Review of p53 Regulation of Oxidative Stress in Skeletal MuscleDocument19 pagesA Systematic Review of p53 Regulation of Oxidative Stress in Skeletal MuscleHugo FalquetoNo ratings yet
- Transforming Pain Medicine (2013)Document17 pagesTransforming Pain Medicine (2013)Hugo FalquetoNo ratings yet
- What Is This Thing Called Pain (2010)Document3 pagesWhat Is This Thing Called Pain (2010)Hugo FalquetoNo ratings yet
- Anticatabolic Effects of Keto BodiesDocument3 pagesAnticatabolic Effects of Keto BodiesHugo FalquetoNo ratings yet
- Neuromodulatory Treatments For Chronic PainDocument12 pagesNeuromodulatory Treatments For Chronic PainHugo FalquetoNo ratings yet
- Cellulite Luebberding2015Document14 pagesCellulite Luebberding2015Hugo FalquetoNo ratings yet
- Neural Adaptation To Resistance TrainingDocument11 pagesNeural Adaptation To Resistance TrainingHugo FalquetoNo ratings yet
- BAAR K. Signals Mediating Skeletal Muscle Remodeling by Resistance Exercise JapplphysiolDocument8 pagesBAAR K. Signals Mediating Skeletal Muscle Remodeling by Resistance Exercise JapplphysiolHugo FalquetoNo ratings yet
- Blood Flow Restriction The Metabolite Volume Threshold Theory (2011)Document5 pagesBlood Flow Restriction The Metabolite Volume Threshold Theory (2011)Hugo FalquetoNo ratings yet
- Bjsports 2017 098391.fullDocument10 pagesBjsports 2017 098391.fullHugo FalquetoNo ratings yet
- Complexity in The Physiotherapy Management of Low Back DisordersDocument5 pagesComplexity in The Physiotherapy Management of Low Back DisordersHugo FalquetoNo ratings yet
- Horizontal and Vertical Jump PDFDocument9 pagesHorizontal and Vertical Jump PDFHugo FalquetoNo ratings yet
- Low Back Pain Research - Future DirectionsDocument10 pagesLow Back Pain Research - Future DirectionsHugo FalquetoNo ratings yet
- Proprioception in Musculoskeletal RehabilitationDocument10 pagesProprioception in Musculoskeletal RehabilitationHugo FalquetoNo ratings yet
- Global Burden of Disease Study 2013Document58 pagesGlobal Burden of Disease Study 2013Anderson SilvaNo ratings yet
- The Use of Vibration As An Exercise Intervention PDFDocument5 pagesThe Use of Vibration As An Exercise Intervention PDFHugo FalquetoNo ratings yet
- Potential Beneficial Effects of Whole-BodyDocument5 pagesPotential Beneficial Effects of Whole-BodyHugo FalquetoNo ratings yet
- Association Between Neck Muscle Coactivation, Pain, and StrengthDocument7 pagesAssociation Between Neck Muscle Coactivation, Pain, and StrengthHugo FalquetoNo ratings yet
- The Role of Spinal Manipulation in Addressing Disordered SensorimotorDocument9 pagesThe Role of Spinal Manipulation in Addressing Disordered SensorimotorHugo FalquetoNo ratings yet
- A Pilot Study of Core Stability and AthleticDocument12 pagesA Pilot Study of Core Stability and AthleticHugo FalquetoNo ratings yet
- A Hypothesis of Chronic Back Pain Ligament Subfailure Injuries Lead To Muscle Control DysfunctionDocument9 pagesA Hypothesis of Chronic Back Pain Ligament Subfailure Injuries Lead To Muscle Control DysfunctionHugo FalquetoNo ratings yet
- Relationship Between Mechanical FactorsDocument15 pagesRelationship Between Mechanical FactorsHugo FalquetoNo ratings yet
- Application of Wellness in Physical TherapyDocument26 pagesApplication of Wellness in Physical TherapyZgama AbdulrahmanNo ratings yet
- Pharmaceutical Study of Pottali Kaplana: Vd.V.RamakrishnaDocument16 pagesPharmaceutical Study of Pottali Kaplana: Vd.V.RamakrishnaRamakrishna Viswanadha67% (3)
- 2022 Seminar Nasional Penelitian dan Pengabdian Kepada Masyarakat (SNPPKM) Focuses on PONV Differences in ERACS and Elective C-Section MethodsDocument6 pages2022 Seminar Nasional Penelitian dan Pengabdian Kepada Masyarakat (SNPPKM) Focuses on PONV Differences in ERACS and Elective C-Section MethodsNers RidaNo ratings yet
- MRCPUK Prospectus WebDocument13 pagesMRCPUK Prospectus WebSen balanNo ratings yet
- Epi#3Document19 pagesEpi#3JNo ratings yet
- GINADocument37 pagesGINArohit vohraNo ratings yet
- Doctors in the New Millennium: Hippocrates or HypocritesDocument28 pagesDoctors in the New Millennium: Hippocrates or HypocritesHaylay GebreyohannesNo ratings yet
- SHN ObjectivesDocument3 pagesSHN Objectivescherie_92989No ratings yet
- HRM Case Study-PatelDocument11 pagesHRM Case Study-PatelHumaira ShafiqNo ratings yet
- طبى 145Document2 pagesطبى 145Yazan AbuFarhaNo ratings yet
- Community Public Health Nursing Practice Health For Families and Populations 5th Edition Maurer Test BankDocument36 pagesCommunity Public Health Nursing Practice Health For Families and Populations 5th Edition Maurer Test Banksejanttrend.hebh7100% (24)
- Principles of Urinary CatheterisationDocument26 pagesPrinciples of Urinary CatheterisationSANU RAMASWAMYNo ratings yet
- HAK DAN KEWAJIBAN PASIEN InggrisDocument1 pageHAK DAN KEWAJIBAN PASIEN Inggrisdewi asnaniNo ratings yet
- J Parenter Enteral Nutr - 2013 - Choban - A S P E N Clinical GuidelinesDocument31 pagesJ Parenter Enteral Nutr - 2013 - Choban - A S P E N Clinical Guidelinescarlos enriqueNo ratings yet
- Director Quality Risk Management in Dallas TX Resume Debra WilliamsDocument5 pagesDirector Quality Risk Management in Dallas TX Resume Debra WilliamsDebra WilliamsNo ratings yet
- Legal Case StudyDocument36 pagesLegal Case StudyJasmine PungginaguinaNo ratings yet
- Ethics in Midwifery PowerpointDocument24 pagesEthics in Midwifery PowerpointEden NatividadNo ratings yet
- Continuous Quality Improvement Cqi Project ProposalDocument6 pagesContinuous Quality Improvement Cqi Project Proposalapi-581690140No ratings yet
- Operational Forces Medical Liaison: Office InformationDocument4 pagesOperational Forces Medical Liaison: Office InformationRicky PermataNo ratings yet
- LocumconsultantgastroJDJan2019Document12 pagesLocumconsultantgastroJDJan2019M LubisNo ratings yet
- Repackaging and Labelling Medicines GuideDocument18 pagesRepackaging and Labelling Medicines GuidetesteNo ratings yet
- Ido PPT 2020Document47 pagesIdo PPT 2020Vikas SinhmarNo ratings yet
- Satairapan Starting Intravenous InfusionDocument3 pagesSatairapan Starting Intravenous InfusionMichelle SatairapanNo ratings yet
- Nursing Practical Guideline Procedure EnemaDocument5 pagesNursing Practical Guideline Procedure EnemaRonny IswahyudiNo ratings yet
- Prescription Event MonitoringDocument19 pagesPrescription Event MonitoringGeethika GummadiNo ratings yet
- Bedside To Boardroom PDFDocument7 pagesBedside To Boardroom PDFDayanaNo ratings yet