You might also like
- Lecture 2-Blood RBC WBCDocument51 pagesLecture 2-Blood RBC WBCsamayaNo ratings yet
- Anph121lb CardiovascularDocument28 pagesAnph121lb CardiovascularDANIELA PEREZNo ratings yet
- Anemia Its Laboratory DiagnosisDocument146 pagesAnemia Its Laboratory DiagnosisCh M MushahidNo ratings yet
- Anaphy Chapter 22 Lymphatic System Doran Mls 1 FDocument10 pagesAnaphy Chapter 22 Lymphatic System Doran Mls 1 FayenaNo ratings yet
- Blood: Blood Is Made Up ofDocument5 pagesBlood: Blood Is Made Up ofNatasha JeanNo ratings yet
- D. Pseudounipolar D. All of The FollowingDocument5 pagesD. Pseudounipolar D. All of The Followingjed larsen capulong gavinoNo ratings yet
- Immune Response ClassDocument55 pagesImmune Response ClassKoushali BanerjeeNo ratings yet
- All Previous Krok ExamsDocument224 pagesAll Previous Krok ExamsOnur KoyuncuNo ratings yet
- HemopoesisDocument31 pagesHemopoesisChandra Shinoda100% (2)
- Dr. Manella Joseph Senior Lecturer/Consultant PathologistDocument41 pagesDr. Manella Joseph Senior Lecturer/Consultant PathologistNipun Shamika100% (1)
- Anatomy and Physiology: Charles Z. Ariola JR, MSN, LPT, Rn. Subject ProfessorDocument124 pagesAnatomy and Physiology: Charles Z. Ariola JR, MSN, LPT, Rn. Subject ProfessorCharlz Zipagan100% (1)
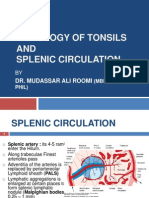
- Histology of Tonsil and Splenic Circulation by Dr. RoomiDocument21 pagesHistology of Tonsil and Splenic Circulation by Dr. RoomiMudassar RoomiNo ratings yet
- Macromolecules WorksheetDocument10 pagesMacromolecules WorksheetShaira BautistaNo ratings yet
- I. Cellular Adaptations:: Cellular Injury, Cell Adaptation & Cell Death 1. Hyperplasia 3. AtrophyDocument4 pagesI. Cellular Adaptations:: Cellular Injury, Cell Adaptation & Cell Death 1. Hyperplasia 3. AtrophyShuaib SiddiquiNo ratings yet
- Cardiovascular System: Anatomy and PhysiologyDocument10 pagesCardiovascular System: Anatomy and PhysiologyDavid PunzalanNo ratings yet
- HIS.K.1.Histology of BloodDocument16 pagesHIS.K.1.Histology of BloodMayaPasaribuNo ratings yet
- Heart Reviewer 1Document6 pagesHeart Reviewer 1tokzzNo ratings yet
- A-P Chapter 4 TissueDocument21 pagesA-P Chapter 4 TissueMONIQUE VELASCONo ratings yet
- Composition and Function of Blood ComponentsDocument17 pagesComposition and Function of Blood ComponentsPrakash Kumar Nayak100% (1)
- 5.0 LeukopoiesisDocument37 pages5.0 LeukopoiesisJunior SataNo ratings yet
- Histology of Male Reproductive SystemDocument3 pagesHistology of Male Reproductive SystemSanna Asila AkramNo ratings yet
- Lymphatic PDFDocument8 pagesLymphatic PDFJoydee Liza MarcoNo ratings yet
- 2-Fertilization & ImplantationDocument20 pages2-Fertilization & ImplantationMochammad Rizal Attamimi0% (1)
- PATHOLOGY Mendelian DisordersDocument8 pagesPATHOLOGY Mendelian DisordersAmna BaigNo ratings yet
- Human Anatomy and PhysiologyDocument8 pagesHuman Anatomy and PhysiologyDanielle AguilaNo ratings yet
- Apoptosis PPT, Pathological AnatomyDocument15 pagesApoptosis PPT, Pathological AnatomyN J3 CNo ratings yet
- White Blood CellsDocument35 pagesWhite Blood CellsYsa ZapantaNo ratings yet
- Female Physiology (Part 2)Document5 pagesFemale Physiology (Part 2)Melissa SalayogNo ratings yet
- Introduction To PathologyDocument35 pagesIntroduction To PathologyBlen AsmeromNo ratings yet
- BloodDocument197 pagesBloodNimesh Sharma100% (1)
- Tissues 4Document65 pagesTissues 4marianisie448100% (3)
- Neoplasm Lecture NotesDocument6 pagesNeoplasm Lecture Notesmiguel gaquitNo ratings yet
- Lymphatic System ExamDocument2 pagesLymphatic System ExamJacobNo ratings yet
- Pathology of Blood and Lymphatic VesselsDocument55 pagesPathology of Blood and Lymphatic VesselsMhinory OctNo ratings yet
- Important Question of PhysiologyDocument8 pagesImportant Question of PhysiologyRahul Yadav100% (2)
- Histology of Spleen by DR Roomi (26!04!12)Document18 pagesHistology of Spleen by DR Roomi (26!04!12)Mudassar Roomi100% (1)
- Necrosis and Degeneration - Copy)Document41 pagesNecrosis and Degeneration - Copy)Saubie Aslamiah100% (2)
- Acute InflammationDocument55 pagesAcute InflammationMohammad_Islam8790% (10)
- Cells and Tissues: 2 Types of Cells That Are Found in The BodyDocument6 pagesCells and Tissues: 2 Types of Cells That Are Found in The BodyAngela ReyesNo ratings yet
- Histology of Synapse and Neuroglia by Dr. RoomiDocument18 pagesHistology of Synapse and Neuroglia by Dr. RoomiMudassar Roomi100% (1)
- Nervous Tissue.: Dr. Zahid Mehmood DPT, MS-NMPTDocument25 pagesNervous Tissue.: Dr. Zahid Mehmood DPT, MS-NMPTZahid Mehmood100% (1)
- ImmunogeneticsDocument46 pagesImmunogeneticsrekha19780% (1)
- As Biochemistry QuizDocument7 pagesAs Biochemistry QuizFati QuaynorNo ratings yet
- Connective TissueDocument7 pagesConnective TissueSheena Pasion100% (1)
- Histology, Lecture 6, Connective Tissues (Lecture Notes)Document6 pagesHistology, Lecture 6, Connective Tissues (Lecture Notes)Ali Al-Qudsi100% (3)
- 1 Edited My Class Note 1 On Blood BankDocument42 pages1 Edited My Class Note 1 On Blood Bankmatewos100% (1)
- Introduction To The Endocrine System NotesDocument12 pagesIntroduction To The Endocrine System NotesJulioNo ratings yet
- Mitosis: Labeled Diagram: Interphase: Gap 1 Phase (Growth), Synthesis Phase (Copy of DNA), Gap 2 Phase (OrganelleDocument7 pagesMitosis: Labeled Diagram: Interphase: Gap 1 Phase (Growth), Synthesis Phase (Copy of DNA), Gap 2 Phase (Organelleazzahra adeliaNo ratings yet
- Introduction To HistologyDocument5 pagesIntroduction To HistologyPau Basco100% (1)
- HemostasisDocument48 pagesHemostasissianturisuryaNo ratings yet
- Reversible Cell Injury and Adaptation (09.11.2017)Document25 pagesReversible Cell Injury and Adaptation (09.11.2017)ISRAELNo ratings yet
- Histology of Nervous Tissue PESTEDocument25 pagesHistology of Nervous Tissue PESTEEd dela PenaNo ratings yet
- BloodDocument6 pagesBloodFadhil Hussam AhmedNo ratings yet
- CNS Physiology LectureDocument25 pagesCNS Physiology Lectureجبار هاوش عضيرس100% (1)
- Biochemistry of Blood Elements: The Figure Is Found at (March 2007)Document37 pagesBiochemistry of Blood Elements: The Figure Is Found at (March 2007)Sadam_fasterNo ratings yet
- Tissues, Glands and MembranesDocument68 pagesTissues, Glands and MembranesMerrylFrancisco100% (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- The Blood and Its ConstituentsDocument71 pagesThe Blood and Its ConstituentsElidadi KatoNo ratings yet
- Blood: Group 1Document25 pagesBlood: Group 1Arian May MarcosNo ratings yet
- 1-Blood Composition and FunctionDocument43 pages1-Blood Composition and FunctionKaleem Mohammad100% (2)
- Orthodontic Pearls PDFDocument2 pagesOrthodontic Pearls PDFortho123No ratings yet
- 9 Fetal Membranes-Dr - GosaiDocument22 pages9 Fetal Membranes-Dr - GosaiDr.B.B.GosaiNo ratings yet
- Principles of Motor DevelopmentDocument15 pagesPrinciples of Motor DevelopmentRina Siason AbaNo ratings yet
- Epilepsy and Pregnancy Gynae Course 2013Document57 pagesEpilepsy and Pregnancy Gynae Course 2013Anas KhanNo ratings yet
- Dialysis Center in BPDHDocument29 pagesDialysis Center in BPDHXien Cadiz100% (5)
- Barry S. Fogel, Donna B. Greenberg-Psychiatric Care of The Medical Patient-Oxford University Press (2015) PDFDocument1,813 pagesBarry S. Fogel, Donna B. Greenberg-Psychiatric Care of The Medical Patient-Oxford University Press (2015) PDFhalamadrid77100% (2)
- PDS Position Paper On Covid Vaccination - Final - 3 7 21Document7 pagesPDS Position Paper On Covid Vaccination - Final - 3 7 21KROPTECK GNo ratings yet
- Katharina Hiria Daundy - Premature Contraction in PregnancyDocument11 pagesKatharina Hiria Daundy - Premature Contraction in PregnancyObgyn AgustusNo ratings yet
- Essentials in Piezosurger Clinical Advantages in Dentistry VercellottiDocument136 pagesEssentials in Piezosurger Clinical Advantages in Dentistry VercellottiayudewintasariNo ratings yet
- Azide Dextrose BrothDocument1 pageAzide Dextrose BrothJHOSELINE KHATERINE RAMIREZ BARBARANNo ratings yet
- New ACR EULAR Guidelines For Systemic Sclerosis ClassificationDocument8 pagesNew ACR EULAR Guidelines For Systemic Sclerosis Classificationadri20121989No ratings yet
- Referat Smile FixfixDocument24 pagesReferat Smile FixfixarumNo ratings yet
- Chap-2 Notes For Clinical Nutrition and DieteticsDocument5 pagesChap-2 Notes For Clinical Nutrition and Dieteticsstar “Hjaljimmer” platinumNo ratings yet
- Alan Immerman - Health Unlimitred PDFDocument95 pagesAlan Immerman - Health Unlimitred PDFHMNo ratings yet
- QSE6034: Teknologi Dan Inovasi Dalam Sains SukanDocument3 pagesQSE6034: Teknologi Dan Inovasi Dalam Sains SukanMohamad Ramlan RamliNo ratings yet
- Vital Signs ObjectivesDocument3 pagesVital Signs ObjectivesJazmin Venice LasalaNo ratings yet
- Test Bank For Equipment Theory For Respiratory Care 5th Edition by WhiteDocument11 pagesTest Bank For Equipment Theory For Respiratory Care 5th Edition by Whiteharoldbrownorcnxeijgd100% (29)
- Step 3 Surgery Uworld NotesDocument11 pagesStep 3 Surgery Uworld Notesaleks patralskaNo ratings yet
- Trelegy and Device InformationDocument40 pagesTrelegy and Device Informationtechang1No ratings yet
- 11 Grammar Test: 94 Photocopiable © Oxford University PressDocument1 page11 Grammar Test: 94 Photocopiable © Oxford University PressLauri RosseNo ratings yet
- DermatologyDocument30 pagesDermatologyCarlos HernándezNo ratings yet
- Feeding Device Shaju V Cherian and Dipu KCDocument20 pagesFeeding Device Shaju V Cherian and Dipu KCShaju V CherianNo ratings yet
- Gender Identity Disorder Not Otherwise SpecifiedDocument4 pagesGender Identity Disorder Not Otherwise SpecifiedJona AddatuNo ratings yet
- Phool Vati BillDocument13 pagesPhool Vati BillVivek PaylaNo ratings yet
- Antiepileptic Drugs ThesisDocument5 pagesAntiepileptic Drugs Thesisfjf8xxz4100% (2)
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaDocument10 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaAsha NopatiNo ratings yet
- Paces Guide 2012 From Online NotesDocument228 pagesPaces Guide 2012 From Online NotesThistell ThistleNo ratings yet
- What Is A Medical Technologist?: History of Medical Technology ProfessionDocument7 pagesWhat Is A Medical Technologist?: History of Medical Technology ProfessionRey Ann ConcepcionNo ratings yet
- Focus Charting of FDocument12 pagesFocus Charting of FLester GonzalesNo ratings yet
- American Board of Family Medicine: TTT SAMPLE TTTDocument148 pagesAmerican Board of Family Medicine: TTT SAMPLE TTTAbdulrhman AlruwiliNo ratings yet