You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Role and Functions of Mental Health NurseDocument20 pagesRole and Functions of Mental Health NurseBinal Joshi86% (7)
- Case Report: A Case Report of Peritoneal Tuberculosis: A Challenging DiagnosisDocument4 pagesCase Report: A Case Report of Peritoneal Tuberculosis: A Challenging DiagnosisDumitru RadulescuNo ratings yet
- Bhagatwala Et Al 2015, Indications and ContraindicationsDocument27 pagesBhagatwala Et Al 2015, Indications and Contraindicationsedo adimastaNo ratings yet
- Conjunctivitis A Systematic Review of Diagnosis and TreatmentDocument18 pagesConjunctivitis A Systematic Review of Diagnosis and TreatmentdasityarachmanNo ratings yet
- Management of Hypertensive Crisis (Diskusi RSUD)Document20 pagesManagement of Hypertensive Crisis (Diskusi RSUD)Kia AgusputraNo ratings yet
- TractionDocument42 pagesTractionThasheela V0% (2)
- Clonazepam Drug CardDocument1 pageClonazepam Drug CardSheri490No ratings yet
- Staphylococcus: Gram Positive CocciDocument3 pagesStaphylococcus: Gram Positive CoccilykaperiasNo ratings yet
- Viral Exanthem ManagementDocument4 pagesViral Exanthem Managementrona ellein galoNo ratings yet
- Acute: Renal Failure Management in The NeonateDocument8 pagesAcute: Renal Failure Management in The NeonatejahangirealamNo ratings yet
- Persistence Market Research: Point of Care Test Market: Global Industry Analysis and Forecast 2016 - 2022Document6 pagesPersistence Market Research: Point of Care Test Market: Global Industry Analysis and Forecast 2016 - 2022api-302003482No ratings yet
- 5 Best Homeopathic Medicine in Urinary Tract InfectionsDocument12 pages5 Best Homeopathic Medicine in Urinary Tract InfectionsVIJAY VATSALNo ratings yet
- Pharma 1 Schools TalkDocument26 pagesPharma 1 Schools TalkEng-MustafaHathalAl-SaraiNo ratings yet
- Sea RemediesDocument2 pagesSea Remedieskaravi schiniasNo ratings yet
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- CHRONIC HEPATITIS Prof DR Tarek ShetaDocument38 pagesCHRONIC HEPATITIS Prof DR Tarek ShetaSheren GamaleldenNo ratings yet
- Translate TineaDocument12 pagesTranslate TineaIndah Permata SariNo ratings yet
- Drug Study NCP - San LazaroDocument9 pagesDrug Study NCP - San LazaroLynne CammayoNo ratings yet
- Food As Medicine: Further Examples of Using Foods As MedicineDocument8 pagesFood As Medicine: Further Examples of Using Foods As MedicineErika UgronNo ratings yet
- Sexual HealthDocument11 pagesSexual Healthapi-236516264No ratings yet
- BBCRDocument40 pagesBBCRmahavir ghiyaNo ratings yet
- C1 Ob-Gyn-2020Document33 pagesC1 Ob-Gyn-2020yabsera mulatuNo ratings yet
- Pneumonia (Pulmonya)Document33 pagesPneumonia (Pulmonya)LopaoMedinaNo ratings yet
- SplenectomyDocument5 pagesSplenectomysharjil chaudhryNo ratings yet
- Keshe - Nano and Gans Health Apps 3of4 29ppDocument29 pagesKeshe - Nano and Gans Health Apps 3of4 29ppExopolitika MagyarországNo ratings yet
- AlbendazoleDocument7 pagesAlbendazolefinchan IrawanNo ratings yet
- Panadeine: What Is in This LeafletDocument3 pagesPanadeine: What Is in This Leafletradzi66No ratings yet
- Enzymes - What The Experts KnowDocument252 pagesEnzymes - What The Experts KnowRocio Uresti De Ramirez0% (1)
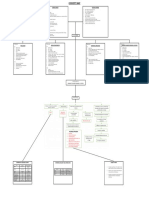
- IM-CAP Concept MapDocument1 pageIM-CAP Concept MapTrisNo ratings yet
- Clinical Practice Guidelines 2021 - Egyptian ORL Society... - Copy-1-185Document185 pagesClinical Practice Guidelines 2021 - Egyptian ORL Society... - Copy-1-185abdalla materNo ratings yet