You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- IV Therapy SsDocument56 pagesIV Therapy Sssaeed_chohan100% (8)
- Eric Berg CVDocument6 pagesEric Berg CVHaralambicNo ratings yet
- Hangnails and HomoeopathyDocument7 pagesHangnails and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Prostho MCQ Www-Matterhere-Com NRRDocument10 pagesProstho MCQ Www-Matterhere-Com NRRYoung FlameNo ratings yet
- Real Estate Rewind Bigger PocketsDocument117 pagesReal Estate Rewind Bigger PocketsspartacuslivesNo ratings yet
- Nursing Home Care Part II Clinical AspectsDocument1 pageNursing Home Care Part II Clinical AspectsspartacuslivesNo ratings yet
- Nursing Home Care Part II Clinical AspectsDocument1 pageNursing Home Care Part II Clinical AspectsspartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Nursing Home Care Part II Clinical AspectsDocument1 pageNursing Home Care Part II Clinical AspectsspartacuslivesNo ratings yet
- Nursing Home Care Part II Clinical AspectsDocument1 pageNursing Home Care Part II Clinical AspectsspartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Sbar Nursing VideoDocument1 pageSbar Nursing VideospartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Sbar Nursing VideoDocument1 pageSbar Nursing VideospartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Critical Thinking in NursingDocument5 pagesCritical Thinking in NursingspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Sbar Nursing VideoDocument1 pageSbar Nursing VideospartacuslivesNo ratings yet
- Ranking of Nutrient Density Scores 2014Document2 pagesRanking of Nutrient Density Scores 2014spartacuslivesNo ratings yet
- Is It DKA or HHSDocument6 pagesIs It DKA or HHSspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Is It DKA or HHSDocument6 pagesIs It DKA or HHSspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Rapid Response Team TrainingDocument3 pagesRapid Response Team TrainingspartacuslivesNo ratings yet
- Is It DKA or HHSDocument6 pagesIs It DKA or HHSspartacuslivesNo ratings yet
- Is It DKA or HHSDocument6 pagesIs It DKA or HHSspartacuslivesNo ratings yet
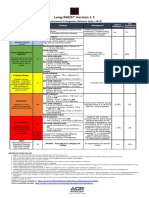
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Penatalaksanaan Penyakit Infeksi Tropik Dengan Ko-Infeksi Covid-19 - Assoc - Prof.dr - Dr. Kurnia Fitri Jamil, M.kes, SP - Pd-Kpti, FinasimDocument33 pagesPenatalaksanaan Penyakit Infeksi Tropik Dengan Ko-Infeksi Covid-19 - Assoc - Prof.dr - Dr. Kurnia Fitri Jamil, M.kes, SP - Pd-Kpti, FinasimFikri FachriNo ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- ACLS NotesDocument3 pagesACLS Notessaxmanwrv0% (1)
- 17-6 eJDD FinalDocument100 pages17-6 eJDD FinalMohamed GamalNo ratings yet
- Bull InfertilDocument29 pagesBull InfertilYonaaasNo ratings yet
- Asthma Attack Nursing Care Plan for Married Female PatientDocument5 pagesAsthma Attack Nursing Care Plan for Married Female PatientMarivic Yuson MalagarNo ratings yet
- Cervical Lymphoepithelial CystDocument6 pagesCervical Lymphoepithelial CystAhmed Al-jumailiNo ratings yet
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesDocument4 pagesChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZNo ratings yet
- Bladder Cancer Types, Symptoms, Tests & TreatmentDocument1 pageBladder Cancer Types, Symptoms, Tests & TreatmentCarmina AguilarNo ratings yet
- Transverse Dimension Diagnosis and Relevance to Functional OcclusionDocument6 pagesTransverse Dimension Diagnosis and Relevance to Functional OcclusionDino MainoNo ratings yet
- Medical Handwashing Procedure StepsDocument3 pagesMedical Handwashing Procedure StepsKERL RAMANo ratings yet
- Amavatha & VathasonithaDocument125 pagesAmavatha & VathasonithaCicil AbrahamNo ratings yet
- CDN 1 PDFDocument22 pagesCDN 1 PDFJohn Mark100% (1)
- Biology 1Document18 pagesBiology 1zaydeeeeNo ratings yet
- Week 29 - DRRRDocument5 pagesWeek 29 - DRRRMira VeranoNo ratings yet
- Lesson 3 ReviewDocument4 pagesLesson 3 ReviewHo Yong WaiNo ratings yet
- Effects of Malnutrition Among ChildrenDocument3 pagesEffects of Malnutrition Among ChildrenDesiree Aranggo MangueraNo ratings yet
- Not Eligible As No Experience of Teaching and ResearchDocument5 pagesNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNo ratings yet
- Electrocardiography Wave Analysis: Using MATLABDocument19 pagesElectrocardiography Wave Analysis: Using MATLABSMNo ratings yet
- Nursing Management - Colon CancerDocument7 pagesNursing Management - Colon CancerReese Alessandra GandulfoNo ratings yet
- Role of Autologous Platelet-Rich Plasma in Z-PlastyDocument3 pagesRole of Autologous Platelet-Rich Plasma in Z-PlastyasclepiuspdfsNo ratings yet
- NSAID's QuestionsDocument3 pagesNSAID's QuestionsManikanta Guptha100% (2)
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamDocument21 pagesChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoNo ratings yet
- Should Medical Marijuana Be Legalized For PatientsDocument4 pagesShould Medical Marijuana Be Legalized For PatientsBing Cossid Quinones CatzNo ratings yet