You might also like
- Bio SurfactantsDocument15 pagesBio SurfactantsherfuentesNo ratings yet
- Guidelines Retail Construction RequirementsDocument25 pagesGuidelines Retail Construction RequirementsherfuentesNo ratings yet
- Practical ContaminationDocument45 pagesPractical ContaminationRagu RajanNo ratings yet
- Guideline For Stability StudiesDocument44 pagesGuideline For Stability StudiesboddarambabuNo ratings yet
- Oxobiodegradable Plastic: An Article by Professor Gerald ScottDocument3 pagesOxobiodegradable Plastic: An Article by Professor Gerald ScottherfuentesNo ratings yet
- Coat HidrofobicoDocument52 pagesCoat HidrofobicoherfuentesNo ratings yet
- Kefir - A Complex ProbioticDocument33 pagesKefir - A Complex ProbioticherfuentesNo ratings yet
- Hydraulic Fracturing FluidsDocument26 pagesHydraulic Fracturing FluidsherfuentesNo ratings yet
- Antimicrobial Products-Test For Antimicrobial Activity and EfficacyDocument14 pagesAntimicrobial Products-Test For Antimicrobial Activity and EfficacyherfuentesNo ratings yet
- 5990 8801EN Hi Plex CompendiumDocument98 pages5990 8801EN Hi Plex CompendiumherfuentesNo ratings yet
- Disinfectants Evaluation GuidelinesDocument44 pagesDisinfectants Evaluation Guidelinesamerican_guy10No ratings yet
- 5990 8801EN Hi Plex CompendiumDocument98 pages5990 8801EN Hi Plex CompendiumherfuentesNo ratings yet
- Screw Extrusion Pretreatments To Enhance The Hydrolysis ofDocument5 pagesScrew Extrusion Pretreatments To Enhance The Hydrolysis ofherfuentesNo ratings yet
- Curing Agents For Epoxy ResinsDocument10 pagesCuring Agents For Epoxy ResinsmombarreNo ratings yet
- SGLS Guide to Oxo-biodegradable PlasticsDocument12 pagesSGLS Guide to Oxo-biodegradable PlasticsherfuentesNo ratings yet
- 8-Final Guidance To RPMS - RES 021610Document50 pages8-Final Guidance To RPMS - RES 021610aditya_asvaNo ratings yet
- Antimicrobial Products-Test For Antimicrobial Activity and EfficacyDocument14 pagesAntimicrobial Products-Test For Antimicrobial Activity and EfficacyherfuentesNo ratings yet
- Stem Cells10 PDFDocument17 pagesStem Cells10 PDFherfuentesNo ratings yet
- Negative Pressure Wound TherapyDocument2 pagesNegative Pressure Wound TherapyherfuentesNo ratings yet
- ImmunoassaysDocument52 pagesImmunoassaysherfuentesNo ratings yet
- Test Skin PDFDocument368 pagesTest Skin PDFherfuentesNo ratings yet
- Actividad EnzimaticDocument11 pagesActividad EnzimaticherfuentesNo ratings yet
- Actividad EnzimaticDocument11 pagesActividad EnzimaticherfuentesNo ratings yet
- Special Report On Injectables PDFDocument8 pagesSpecial Report On Injectables PDFherfuentesNo ratings yet
- Insect Repellents ReportDocument46 pagesInsect Repellents ReportherfuentesNo ratings yet
- Clean Room PharmaDocument39 pagesClean Room PharmadurbcomsonoNo ratings yet
- zx94092538 05Document14 pageszx94092538 05Chenchen HanNo ratings yet
- Ucm 072450Document35 pagesUcm 072450herfuentesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Paraphrasing: How, Tips, ExamplesDocument9 pagesParaphrasing: How, Tips, ExamplesMahesh RamesNo ratings yet
- MED - Post Review ExamDocument8 pagesMED - Post Review ExamFrederick BallesterosNo ratings yet
- TriageDocument42 pagesTriageNic JiNo ratings yet
- LeprosyDocument9 pagesLeprosyJohn Ribu Parampil100% (1)
- 8 Emergency Formative Clinical Evaluation ChecklistDocument1 page8 Emergency Formative Clinical Evaluation Checklistمهند الرحيليNo ratings yet
- ISOFLURANE anaesthesia data sheetDocument5 pagesISOFLURANE anaesthesia data sheetChristian James CamaongayNo ratings yet
- Power and Empowerment in NursingDocument40 pagesPower and Empowerment in NursingPabasara AmarasingheNo ratings yet
- Maintain AirwaysDocument3 pagesMaintain AirwaysJei JayNo ratings yet
- Journal Prosto PDFDocument6 pagesJournal Prosto PDFdifaNo ratings yet
- Vaginal Yeast InfectionsDocument7 pagesVaginal Yeast InfectionsAnimesh PriyaNo ratings yet
- Megan Talbott ResumeDocument3 pagesMegan Talbott Resumeapi-291314145No ratings yet
- Nurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanDocument5 pagesNurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanEmma WatsonNo ratings yet
- Case Report Consent Form TemplateDocument2 pagesCase Report Consent Form TemplateDaniel Antonio Valderrama Merejildo100% (1)
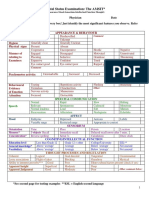
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 pagesMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Basic Airway ManagementDocument98 pagesBasic Airway ManagementRani Salsabilah100% (1)
- Narrative Report On School Nursing - EditedDocument16 pagesNarrative Report On School Nursing - EditedAbby_Cacho_9151100% (2)
- AllDocument48 pagesAllnanchieNo ratings yet
- Managing Impaired Gas Exchange and Ineffective Airway ClearanceDocument27 pagesManaging Impaired Gas Exchange and Ineffective Airway ClearancecuakialyannaNo ratings yet
- Pediatrics Pediatrics Pediatrics Pediatrics Pediatrics: Pediatrics Pediatrics Pediatrics Pediatrics PediatricsDocument2 pagesPediatrics Pediatrics Pediatrics Pediatrics Pediatrics: Pediatrics Pediatrics Pediatrics Pediatrics PediatricsBobet Reña100% (2)
- IV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneDocument2 pagesIV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneNdalilashiwa Penehafo Ndakondja-VictorNo ratings yet
- Digital Universe Healthcare Vertical Report ArDocument16 pagesDigital Universe Healthcare Vertical Report ArAmrNo ratings yet
- Neuropathy News ReportDocument4 pagesNeuropathy News ReportMichael R. Beringer100% (1)
- Neural Structures Involved in The Control of MovementDocument68 pagesNeural Structures Involved in The Control of MovementSAYAN NAGNo ratings yet
- History Back PainDocument3 pagesHistory Back PaindrwiraNo ratings yet
- ICNCDRS Blindness Registry FormDocument4 pagesICNCDRS Blindness Registry FormAprilAngeliRobleNo ratings yet
- AOTA Adaptation To Macular Escotomas in Persons With Low VisionDocument7 pagesAOTA Adaptation To Macular Escotomas in Persons With Low VisionadelitaperezNo ratings yet
- Parotid Tumors and Other Salivary Gland TumorsDocument41 pagesParotid Tumors and Other Salivary Gland Tumorsdrhiwaomer100% (9)
- Literature Review For Specimen Labeling and Blood BankDocument3 pagesLiterature Review For Specimen Labeling and Blood Bankapi-236445988No ratings yet
- SOAP Handout 2010Document4 pagesSOAP Handout 2010wawanNo ratings yet
- Disclosures: Kori Dewing, DNP, ARNP Virginia Mason Medical Center October 29, 2013Document3 pagesDisclosures: Kori Dewing, DNP, ARNP Virginia Mason Medical Center October 29, 2013Alexander Diaz ZuletaNo ratings yet