You might also like
- 2012 Aug IMG Poster 165760a SepsisDocument1 page2012 Aug IMG Poster 165760a SepsisTeng Huei LeeNo ratings yet
- Pocket Guide June2013 PDFDocument2 pagesPocket Guide June2013 PDFSergeyGruntov100% (1)
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocument78 pagesVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- OS217 LEC06 Rational Antibiotic UseDocument6 pagesOS217 LEC06 Rational Antibiotic Usegenerics54321No ratings yet
- (CV2) Pharmacology of AnticoagulantsDocument6 pages(CV2) Pharmacology of AnticoagulantsHanifa Shereen B. AliNo ratings yet
- Empiric Treatment Guidelines Common InfectionsDocument9 pagesEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Document48 pagesNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Drugs in Blood DisordersDocument1 pageDrugs in Blood DisordersSantosh patelNo ratings yet
- Classification of DrugsDocument10 pagesClassification of DrugsSafura IjazNo ratings yet
- Klasifikasi Dan Mekanisme ABDocument8 pagesKlasifikasi Dan Mekanisme ABDeboyjackNo ratings yet
- NHS Antibiotice PDFDocument2 pagesNHS Antibiotice PDFHoratiu OanaNo ratings yet
- Antibiotics 101Document49 pagesAntibiotics 101Tony VoNo ratings yet
- Penicinillase - Sensible: Inhibit Clasification AntibioticsDocument1 pagePenicinillase - Sensible: Inhibit Clasification AntibioticsАндрій ДанильцівNo ratings yet
- Nephrotic and NephriticDocument27 pagesNephrotic and Nephritictam meiNo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezNo ratings yet
- EDT007Document110 pagesEDT007mahchusNo ratings yet
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocument5 pagesPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNo ratings yet
- Pharmacology Notes (Chapter 20 and 21)Document2 pagesPharmacology Notes (Chapter 20 and 21)graycorypNo ratings yet
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDocument26 pagesA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- Drug Side EffectsDocument2 pagesDrug Side EffectsAngelic khanNo ratings yet
- Treatment of Chronic Heart FailureDocument2 pagesTreatment of Chronic Heart FailureShannon RamsumairNo ratings yet
- Primary Care Antibiotic Guideline FINAL May 2015Document10 pagesPrimary Care Antibiotic Guideline FINAL May 2015Atta Muhammad MemonNo ratings yet
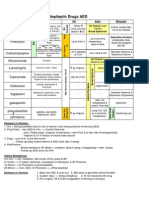
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Meds For HypertensionDocument3 pagesMeds For HypertensionZonicsNo ratings yet
- Antibiotic TableDocument5 pagesAntibiotic TableLiana Et Murat KalabalikNo ratings yet
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDocument16 pagesThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- AntibioticsDocument4 pagesAntibioticsTan Geok Eng100% (1)
- Abx FinalDocument3 pagesAbx Finalyanks1120No ratings yet
- Antibiotics NotesDocument7 pagesAntibiotics NotesmuhammadridhwanNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Beta Lactam AntibioticsDocument1 pageBeta Lactam AntibioticsCourtney TownsendNo ratings yet
- KDT Only ClassificationsDocument72 pagesKDT Only ClassificationsDebashis ParidaNo ratings yet
- Farmakokinetika Klinik Vancomycin: Riri Tifani 1201108Document21 pagesFarmakokinetika Klinik Vancomycin: Riri Tifani 1201108Rahmatul HusnaNo ratings yet
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- Resuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaDocument44 pagesResuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaAna AgustinaNo ratings yet
- Trials SummaryDocument12 pagesTrials SummaryReda SoNo ratings yet
- Antibacterial Drugs SummaryDocument13 pagesAntibacterial Drugs SummaryNeo Ramagaga100% (1)
- With Dr. Susan Lipsett: Community Acquired PneumoniaDocument1 pageWith Dr. Susan Lipsett: Community Acquired PneumoniaJayantiNo ratings yet
- Classification of The DrugsDocument50 pagesClassification of The DrugsGlena SalamNo ratings yet
- Pharmacology A - Drugs Used in Coagulation CascadeDocument13 pagesPharmacology A - Drugs Used in Coagulation CascadeselflessdoctorNo ratings yet
- Antibiotic GuideDocument6 pagesAntibiotic GuideAnnTran100% (1)
- Pharm Expansion 17 NDFDocument1 pagePharm Expansion 17 NDFNokz M. Raki-inNo ratings yet
- DRUG of CHOICE - InfectiousDocument1 pageDRUG of CHOICE - InfectiousJoseph De JoyaNo ratings yet
- Pharmacology (1) - 104-122Document19 pagesPharmacology (1) - 104-122Dental LecturesMMQNo ratings yet
- Vancomycin Auc With Answers 1Document64 pagesVancomycin Auc With Answers 1api-493355126No ratings yet
- PCOL Maps PDFDocument11 pagesPCOL Maps PDFZinc YuloNo ratings yet
- UAW Respiratory Antimicrobial Pharm Guide MedstuDocument19 pagesUAW Respiratory Antimicrobial Pharm Guide MedstuNabeel ShahzadNo ratings yet
- Pharmacology A - NSAIDSDocument14 pagesPharmacology A - NSAIDSselflessdoctorNo ratings yet
- 01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFDocument26 pages01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFawinsyNo ratings yet
- Pharmacology of DiureticsDocument75 pagesPharmacology of DiureticsAhmed BassettNo ratings yet
- Pain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Document3 pagesPain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Ryan TurnerNo ratings yet
- Pharmacology of AntimycobacterialDocument7 pagesPharmacology of Antimycobacterialselflessdoctor100% (1)
- Therapeutic Hypothermia Niraj BharuchDocument31 pagesTherapeutic Hypothermia Niraj BharuchNiraj GuptaNo ratings yet
- Journal Reading EMPEROR-ReducedDocument21 pagesJournal Reading EMPEROR-ReducedLolii Con Harhazyuku100% (1)
- PHM - Hematologic DrugsDocument3 pagesPHM - Hematologic DrugsJeanne Rodiño100% (3)
- THE RELATIONSHIP OF BODY MASS INDEX AND HYPOALBUMINEMIA WITH INFECTION IN GERIATRIC POPULATION AbstrackDocument1 pageTHE RELATIONSHIP OF BODY MASS INDEX AND HYPOALBUMINEMIA WITH INFECTION IN GERIATRIC POPULATION AbstrackAnonymous s4yarxNo ratings yet
- Correlation of BODY MASS INDEX AND ALBUMIN WITH INFECTION IN GERIATRIC POPULATION AbstrackDocument1 pageCorrelation of BODY MASS INDEX AND ALBUMIN WITH INFECTION IN GERIATRIC POPULATION AbstrackAnonymous s4yarxNo ratings yet
- Correlation Between Depression and Falls Among Elderly Patient Hospitalized at Geriatric Ward in Sanglah HospitalDocument1 pageCorrelation Between Depression and Falls Among Elderly Patient Hospitalized at Geriatric Ward in Sanglah HospitalAnonymous s4yarxNo ratings yet
- AGE BODY MASS INDEX AND ALBUMIN in Hospitalized Elderlty Abstrack Penelitian 2 ExtendedDocument4 pagesAGE BODY MASS INDEX AND ALBUMIN in Hospitalized Elderlty Abstrack Penelitian 2 ExtendedAnonymous s4yarxNo ratings yet
- Penelitian Sri Rejeki-Correlation of Sepsis and Albumin SerumDocument1 pagePenelitian Sri Rejeki-Correlation of Sepsis and Albumin SerumAnonymous s4yarxNo ratings yet
- Correlation of BODY MASS INDEX AND ALBUMIN WITH INFECTION IN GERIATRIC POPULATION AbstrackDocument1 pageCorrelation of BODY MASS INDEX AND ALBUMIN WITH INFECTION IN GERIATRIC POPULATION AbstrackAnonymous s4yarxNo ratings yet
- Pneumonia NosokomialDocument29 pagesPneumonia NosokomialAngela NovanthiaNo ratings yet
- ATS GuidelinesDocument46 pagesATS Guidelinesapi-3847280100% (1)
- AGE BODY MASS INDEX AND ALBUMIN in Hospitalized Elderlty Abstrack Penelitian 2Document1 pageAGE BODY MASS INDEX AND ALBUMIN in Hospitalized Elderlty Abstrack Penelitian 2Anonymous s4yarxNo ratings yet
- New Targets in Malaria Parasite Chemotherapy A Review TropikDocument6 pagesNew Targets in Malaria Parasite Chemotherapy A Review TropikAnonymous s4yarxNo ratings yet
- Infdis - Jiv365.full TropikDocument3 pagesInfdis - Jiv365.full TropikAnonymous s4yarxNo ratings yet
- DR Dewi Dian Early Detection of Bacterial Infection in Acute Febrile IllnessDocument9 pagesDR Dewi Dian Early Detection of Bacterial Infection in Acute Febrile IllnessAnonymous s4yarxNo ratings yet
- For Practitioner: Jaundice Obstructive SyndromDocument5 pagesFor Practitioner: Jaundice Obstructive SyndromArsy Mira PertiwiNo ratings yet
- Jurnal Kriteria Baru SleDocument10 pagesJurnal Kriteria Baru SleDr Edi HidayatNo ratings yet
- Nilai Workshop BagusDocument2 pagesNilai Workshop BagusAnonymous s4yarxNo ratings yet
- DHF 1 PDFDocument7 pagesDHF 1 PDFPutriIndahNo ratings yet
- Infdis - Jiv365.full TropikDocument3 pagesInfdis - Jiv365.full TropikAnonymous s4yarxNo ratings yet
- DR Dewi Dian Early Detection of Bacterial Infection in Acute Febrile IllnessDocument9 pagesDR Dewi Dian Early Detection of Bacterial Infection in Acute Febrile IllnessAnonymous s4yarxNo ratings yet
- Prof Tuty The Etiology of Acute Febrile Illness Requiring Hospitalization - Docx2Document3 pagesProf Tuty The Etiology of Acute Febrile Illness Requiring Hospitalization - Docx2Anonymous s4yarxNo ratings yet
- Ectopic Cervical Thyroid Carcinoma-Review of The Literature With Illustrative Case SeriesDocument8 pagesEctopic Cervical Thyroid Carcinoma-Review of The Literature With Illustrative Case SeriesAnonymous s4yarxNo ratings yet
- DR Agus Specimen CultureDocument2 pagesDR Agus Specimen CultureAnonymous s4yarxNo ratings yet
- MAKALAH LENGKAP BIDS-6 Final Abstrak Siap PrintDocument14 pagesMAKALAH LENGKAP BIDS-6 Final Abstrak Siap PrintAnonymous s4yarxNo ratings yet
- JURNAL Uni CoverageDocument11 pagesJURNAL Uni CoverageAnonymous s4yarxNo ratings yet
- JURNAL Uni CoverageDocument11 pagesJURNAL Uni CoverageAnonymous s4yarxNo ratings yet
- JURNAL Uni CoverageDocument11 pagesJURNAL Uni CoverageAnonymous s4yarxNo ratings yet
- JURNAL Uni CoverageDocument11 pagesJURNAL Uni CoverageAnonymous s4yarxNo ratings yet
- Jurnal KeperawatanDocument9 pagesJurnal KeperawatanDewa DiningratNo ratings yet
- Highway-And-Railroad-Engineering SummaryDocument15 pagesHighway-And-Railroad-Engineering SummaryRodin James GabrilloNo ratings yet
- ZF-FreedomLine TransmissionDocument21 pagesZF-FreedomLine TransmissionHerbert M. Zayco100% (1)
- Arduino Oscilloscope ProjectDocument12 pagesArduino Oscilloscope ProjectSathya Narayan100% (1)
- The Acceptability of Rubber Tree Sap (A As An Alternative Roof SealantDocument7 pagesThe Acceptability of Rubber Tree Sap (A As An Alternative Roof SealantHannilyn Caldeo100% (2)
- Significance of GodboleDocument5 pagesSignificance of GodbolehickeyvNo ratings yet
- CBSE DetailsDocument6 pagesCBSE DetailsNARESH KUMARNo ratings yet
- Flight Vehicle Design:: Example 2 (Uav)Document43 pagesFlight Vehicle Design:: Example 2 (Uav)Anmol KumarNo ratings yet
- Lecture 12Document8 pagesLecture 12Mechanical ZombieNo ratings yet
- Emw 2007 FP 02093Document390 pagesEmw 2007 FP 02093boj87No ratings yet
- Ham Radio Balu N ManualDocument7 pagesHam Radio Balu N Manualcolinbeeforth100% (1)
- Douluo Dalu Volume 05 - Star Dou Forest PDFDocument141 pagesDouluo Dalu Volume 05 - Star Dou Forest PDFRay Joseph LealNo ratings yet
- EPCC Hydrocarbon Downstream L&T 09.01.2014Document49 pagesEPCC Hydrocarbon Downstream L&T 09.01.2014shyaminannnaNo ratings yet
- Honeycomb Kevlar 49 (Hexcel)Document3 pagesHoneycomb Kevlar 49 (Hexcel)Julia GarciaNo ratings yet
- Lesson Plan in Science 9: I. ObjectivesDocument8 pagesLesson Plan in Science 9: I. ObjectivesmarichuNo ratings yet
- Lec 4 - 4th WeekDocument40 pagesLec 4 - 4th Weekrajpoot aliNo ratings yet
- Manual PipsDocument5 pagesManual PipsOzzyNo ratings yet
- DudjDocument4 pagesDudjsyaiful rinantoNo ratings yet
- Dawn of Solar PV CookingDocument5 pagesDawn of Solar PV CookingAbhinav AgrawalNo ratings yet
- Faa Registry: N-Number Inquiry ResultsDocument3 pagesFaa Registry: N-Number Inquiry Resultsolga duqueNo ratings yet
- 1962 Gibson Johnny SmithDocument5 pages1962 Gibson Johnny SmithLuisNo ratings yet
- Native Data Sheet Asme b73.1Document4 pagesNative Data Sheet Asme b73.1Akhmad Faruq Alhikami100% (1)
- The Indian Mining Sector: Effects On The Environment & FDI InflowsDocument10 pagesThe Indian Mining Sector: Effects On The Environment & FDI InflowsMehul MandanakaNo ratings yet
- H107en 201906 r4 Elcor Elcorplus 20200903 Red1Document228 pagesH107en 201906 r4 Elcor Elcorplus 20200903 Red1mokbelNo ratings yet
- Combined Shear and TensionDocument16 pagesCombined Shear and TensionDAN MARK OPONDANo ratings yet
- 123 09-Printable Menu VORDocument2 pages123 09-Printable Menu VORArmstrong TowerNo ratings yet
- Math COT 3Document18 pagesMath COT 3Icy Mae SenadosNo ratings yet
- Considerations For Impeller Trimming - Empowering Pumps and EquipmentDocument8 pagesConsiderations For Impeller Trimming - Empowering Pumps and Equipment김기준No ratings yet
- Owner'S Manual: 2023 Chassis CabDocument444 pagesOwner'S Manual: 2023 Chassis CabDmitry DimasNo ratings yet
- Immigrant Italian Stone CarversDocument56 pagesImmigrant Italian Stone Carversglis7100% (2)
- Determinants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Document3 pagesDeterminants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Apurv ChitranshNo ratings yet