You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- PNF PatternsDocument19 pagesPNF PatternsDany VirgilNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Assessment of The Lower LimbDocument496 pagesAssessment of The Lower Limbkacheren100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Volume 15, Number 5 May 2011Document188 pagesVolume 15, Number 5 May 2011Nicolai BabaliciNo ratings yet
- Surgery NotesDocument200 pagesSurgery NotesJasneet SinghNo ratings yet
- GLUCOSE TOLERANCE TEST GUIDEDocument12 pagesGLUCOSE TOLERANCE TEST GUIDEshiv gautamNo ratings yet
- High Resolution CT of The Lung Patterns of Disease and Differential DiagnosesDocument30 pagesHigh Resolution CT of The Lung Patterns of Disease and Differential DiagnosesNicolai Babalici100% (1)
- Understanding Laryngopharyngeal Reflux DiseaseDocument30 pagesUnderstanding Laryngopharyngeal Reflux Diseaseamitkulkarni83100% (1)
- Operations Management 6th Edition Reid Solutions ManualDocument3 pagesOperations Management 6th Edition Reid Solutions Manuala288884902No ratings yet
- FINALS TheoreticalDocument6 pagesFINALS TheoreticalCarol Neng Calupitan100% (1)
- Trypanosomiasis & LeishmaniasisDocument50 pagesTrypanosomiasis & LeishmaniasisMardoni Efrijon75% (4)
- Jupiter EngDocument34 pagesJupiter EngakukauakuNo ratings yet
- Lymphangioleiomyomatosis A Clinical Update ChestDocument12 pagesLymphangioleiomyomatosis A Clinical Update ChestNicolai BabaliciNo ratings yet
- OnchiectasisDocument33 pagesOnchiectasisNicolai BabaliciNo ratings yet
- Lect4 RespiratoryDocument55 pagesLect4 RespiratoryNicolai BabaliciNo ratings yet
- Volume 15, Number 4 April 2011Document162 pagesVolume 15, Number 4 April 2011Nicolai BabaliciNo ratings yet
- Volume 15, Number 6 June 2011Document183 pagesVolume 15, Number 6 June 2011Nicolai BabaliciNo ratings yet
- Volume 15, Number 1 January 2011Document233 pagesVolume 15, Number 1 January 2011Nicolai BabaliciNo ratings yet
- Volume 15, Number 3 March 2011Document152 pagesVolume 15, Number 3 March 2011Nicolai BabaliciNo ratings yet
- Volume 15, Number 2 February 2011Document154 pagesVolume 15, Number 2 February 2011Nicolai BabaliciNo ratings yet
- Volume 15, Number 2 February 2011Document154 pagesVolume 15, Number 2 February 2011Nicolai BabaliciNo ratings yet
- Volume 15, Number 1 January 2011Document233 pagesVolume 15, Number 1 January 2011Nicolai BabaliciNo ratings yet
- Vascular Physiology 3Document39 pagesVascular Physiology 3Nicolai BabaliciNo ratings yet
- Freud Constructions in AnalysisDocument9 pagesFreud Constructions in AnalysisyaelfridNo ratings yet
- Shoulder Assessment Guide for PhysiotherapistsDocument17 pagesShoulder Assessment Guide for PhysiotherapistsNehaNo ratings yet
- Hospital ManagementDocument20 pagesHospital ManagementGokulNo ratings yet
- 10 Nursing Note SampleDocument1 page10 Nursing Note Sampletesttest testNo ratings yet
- 8 Emergency Formative Clinical Evaluation ChecklistDocument1 page8 Emergency Formative Clinical Evaluation Checklistمهند الرحيليNo ratings yet
- Coley 2019Document8 pagesColey 2019KaniNo ratings yet
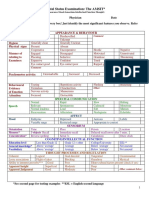
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 pagesMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- October 2017 Ophthalmic PearlsDocument3 pagesOctober 2017 Ophthalmic PearlsShafa KhansaNo ratings yet
- 2014 AHA/ACC Guidelines for Managing NSTE-ACSDocument46 pages2014 AHA/ACC Guidelines for Managing NSTE-ACSEmmieNo ratings yet
- Thoracic Trauma: The Deadly DozenDocument20 pagesThoracic Trauma: The Deadly DozenPANTS1No ratings yet
- Distalization of Maxillary Molars Using A Lever Arm and Mini-ImplantDocument10 pagesDistalization of Maxillary Molars Using A Lever Arm and Mini-ImplantYury Tenorio CahuanaNo ratings yet
- Healthcare Solutions-CooperDocument188 pagesHealthcare Solutions-Cooper7alejandro7No ratings yet
- Referral Counseling - List For WebsiteDocument3 pagesReferral Counseling - List For Websiteapi-425649572No ratings yet
- Increased ICP and Neurological Trauma GuideDocument14 pagesIncreased ICP and Neurological Trauma GuideMhoy CostesNo ratings yet
- Oxy CadDocument21 pagesOxy CadrlinaoNo ratings yet
- Pelvic Fractures ManagementDocument24 pagesPelvic Fractures ManagementSerenna DehalooNo ratings yet
- Case Presentation - Closed Fracture Radius Ulna PediatricDocument30 pagesCase Presentation - Closed Fracture Radius Ulna PediatriciamboredtiredNo ratings yet
- 6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportDocument8 pages6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportkochikaghochiNo ratings yet
- History Back PainDocument3 pagesHistory Back PaindrwiraNo ratings yet
- Diet and NutritionDocument92 pagesDiet and NutritionSheeba AnilNo ratings yet
- CFS - Denigration by DesignDocument246 pagesCFS - Denigration by Designfatima110No ratings yet
- Psychiatry IntroductionDocument26 pagesPsychiatry IntroductionMunir AhmedNo ratings yet