You might also like
- Essential Mineral NutritionDocument13 pagesEssential Mineral NutritionAashishNo ratings yet
- Dynamics of Blood & Lymph FlowDocument35 pagesDynamics of Blood & Lymph FlowVera Arista100% (1)
- Interpret Your Lab ReportsDocument30 pagesInterpret Your Lab ReportspeibNo ratings yet
- MKR Rental ApplicationDocument3 pagesMKR Rental ApplicationWoofWoofJGNo ratings yet
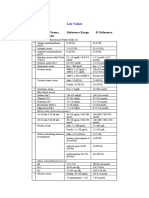
- Blood, Plasma, Serum Reference Range SI Reference: Lab ValuesDocument4 pagesBlood, Plasma, Serum Reference Range SI Reference: Lab ValuesEvaG2012No ratings yet
- A To Z Medical TerminologyDocument16 pagesA To Z Medical TerminologyBobNathanaelNo ratings yet
- Stress Management: Using Self-Help Techniques For Dealing With StressDocument11 pagesStress Management: Using Self-Help Techniques For Dealing With StressCatherine Raymundo MartinezNo ratings yet
- GSM Alternative and Complemantary TherapiesDocument98 pagesGSM Alternative and Complemantary TherapiesMonika shankarNo ratings yet
- HandbookofchemistrylabreagentJ PDFDocument102 pagesHandbookofchemistrylabreagentJ PDFViraj LmgNo ratings yet
- Composition of FaecesmDocument20 pagesComposition of FaecesmnfacmaNo ratings yet
- RenalSystem Part 1 (Spring2020)Document49 pagesRenalSystem Part 1 (Spring2020)Sahil ParikhNo ratings yet
- List of cranial nerves and their functionsDocument2 pagesList of cranial nerves and their functionsKay Lumpas Cruda100% (1)
- Reference Ranges For Blood TestsDocument38 pagesReference Ranges For Blood TestscatalinNo ratings yet
- SerotoninDocument1 pageSerotoninEdwin MartinezNo ratings yet
- Moving Coil Galvanometer - Working, Principle, Construction, Advantages PDFDocument8 pagesMoving Coil Galvanometer - Working, Principle, Construction, Advantages PDFAdityaNo ratings yet
- MedicineDocument21 pagesMedicineAqilah MansorNo ratings yet
- Physical Characteristics of UrineDocument36 pagesPhysical Characteristics of Urinemuhammad saad100% (1)
- Biomedx Studio Software GuideDocument23 pagesBiomedx Studio Software Guidebiomedx100% (1)
- Dhona Balance001Document1 pageDhona Balance001nitinNo ratings yet
- UG Physiology PDFDocument38 pagesUG Physiology PDFAmaradeepika JagannathanNo ratings yet
- Bioptron Colour 25Document34 pagesBioptron Colour 25diNo ratings yet
- 62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseDocument69 pages62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseTarek TarekNo ratings yet
- Advanced MicrosDocument52 pagesAdvanced MicrosLavanya Kalapala100% (1)
- Trauma Nursing IntroductionDocument12 pagesTrauma Nursing Introductionanimesh pandaNo ratings yet
- Acetylcholine Bioassay MethodsDocument1 pageAcetylcholine Bioassay MethodsSangi RajNo ratings yet
- Dietary Reference Intakes (DRIs)Document11 pagesDietary Reference Intakes (DRIs)NathalieCaracaNo ratings yet
- Human Circulatory SystemDocument3 pagesHuman Circulatory SystemRahul Ecka100% (1)
- The A1C Test and DiabetesDocument12 pagesThe A1C Test and Diabetesمحمد عبداللهNo ratings yet
- 10 Blood Tests For Vegans & VegetariansDocument3 pages10 Blood Tests For Vegans & VegetariansWeb WorldNo ratings yet
- Detoxing: Karen Sabetan Certified Nutrition Consultant and Health and Wellness CoachDocument24 pagesDetoxing: Karen Sabetan Certified Nutrition Consultant and Health and Wellness CoachSveta MansmannNo ratings yet
- Syllabus SWS 3022 Online Fall 2017Document13 pagesSyllabus SWS 3022 Online Fall 2017Bethany KellyNo ratings yet
- Suzie BiofeedbackSDCRIDocument3 pagesSuzie BiofeedbackSDCRIocortezlariosNo ratings yet
- Questions Metabolic AcidosisDocument6 pagesQuestions Metabolic Acidosisyayooo2004No ratings yet
- Brainchange: Grea T D Oor ChinaDocument4 pagesBrainchange: Grea T D Oor ChinaJack CarneyNo ratings yet
- BSChem-Statistics in Chemical Analysis PDFDocument6 pagesBSChem-Statistics in Chemical Analysis PDFKENT BENEDICT PERALESNo ratings yet
- Urine AnalysisDocument63 pagesUrine AnalysisVench DemicaisNo ratings yet
- Maintaining Fluid and Electrolyte BalanceDocument137 pagesMaintaining Fluid and Electrolyte BalanceNano Baddour100% (1)
- The Effect of Piezoelectric and Magnetostrictive Scaling DevicesDocument38 pagesThe Effect of Piezoelectric and Magnetostrictive Scaling Devicesnotaden1849No ratings yet
- Non-Essential Amino Acids Nitrogen MetabolismDocument21 pagesNon-Essential Amino Acids Nitrogen Metabolismpradeep36No ratings yet
- Examination of Cranial NervesDocument7 pagesExamination of Cranial NervesrajtanniruNo ratings yet
- Perform Urine Analysis LabDocument116 pagesPerform Urine Analysis LabDr Sumant SharmaNo ratings yet
- Ayurvedic Treatment of Enlarged Prostate GlandDocument28 pagesAyurvedic Treatment of Enlarged Prostate GlandRajeshKizziNo ratings yet
- Liver Protocol 14 PDFDocument4 pagesLiver Protocol 14 PDFapi-390240132No ratings yet
- Cranial Electrotherapy Stimulation: Its First Fifty Years, Plus ThreeDocument36 pagesCranial Electrotherapy Stimulation: Its First Fifty Years, Plus ThreeSilambarasu KaruppiahNo ratings yet
- Grounding Body 2000Document6 pagesGrounding Body 2000TorentSpyNo ratings yet
- BIOL 2900 Learning OutcomesDocument11 pagesBIOL 2900 Learning OutcomesTalk To MeNo ratings yet
- The Medical Medium Cleanse - The Word of SpiritDocument2 pagesThe Medical Medium Cleanse - The Word of SpiritMariaNo ratings yet
- Checklist of Requirements For Acupuncture Certification For Filipino Applicants - V06302015Document1 pageChecklist of Requirements For Acupuncture Certification For Filipino Applicants - V06302015kggggdNo ratings yet
- Heat Shock ProteinsDocument98 pagesHeat Shock ProteinsAprianie Wiwin100% (1)
- Safemedicate Learner Guide UK v2RDocument49 pagesSafemedicate Learner Guide UK v2Rlesky17No ratings yet
- Learn More About Puristat's All-Natural Colon Cleanse : by Jo JordanDocument8 pagesLearn More About Puristat's All-Natural Colon Cleanse : by Jo JordanMahitha ReddyNo ratings yet
- Extraction and Characterization of Guava Seed Oil - A Novel Industrial ByproducDocument9 pagesExtraction and Characterization of Guava Seed Oil - A Novel Industrial ByproducDevita AmeliaNo ratings yet
- ProjectDocument31 pagesProjectShubhamNo ratings yet
- Personal Protective Grounding - Training PresentationDocument31 pagesPersonal Protective Grounding - Training PresentationIrfan UllahNo ratings yet
- Mold Toxins Richard Loyd MDDocument4 pagesMold Toxins Richard Loyd MDOliver QueenNo ratings yet
- 4 Phases of IV Fluid Therapy FinalDocument29 pages4 Phases of IV Fluid Therapy FinalLuqmanul Hakim Junaidden100% (1)
- Improve Your Energy Balance by Adding Dairy and ExerciseDocument8 pagesImprove Your Energy Balance by Adding Dairy and ExercisealafiaNo ratings yet
- Section ADocument25 pagesSection ABobbiNo ratings yet
- Nursing Care Health Assessment Form: Instructions For CompletionDocument6 pagesNursing Care Health Assessment Form: Instructions For CompletionJM RomiasNo ratings yet
- Nursing Care Health Assessment FormDocument5 pagesNursing Care Health Assessment FormMelanie Bagasol SisonNo ratings yet
- ThreeDocument1 pageThreeAnkushNo ratings yet
- LCD Display PICsDocument1 pageLCD Display PICsAnkushNo ratings yet
- Temp CalDocument4 pagesTemp CalAnkushNo ratings yet
- Who I Am - Finding Your IdentityDocument1 pageWho I Am - Finding Your IdentityAnkushNo ratings yet
- AttitudeDocument2 pagesAttitudeAnkushNo ratings yet
- TutorialDocument1 pageTutorialAnkushNo ratings yet
- LCD Display PICsDocument1 pageLCD Display PICsAnkushNo ratings yet
- HrmsDocument1 pageHrmsAnkushNo ratings yet
- Chapter 6. FeverDocument19 pagesChapter 6. FeverMonica CiorneiNo ratings yet
- Hospital Job DescriptionsDocument48 pagesHospital Job DescriptionsLoresita Amoranto Rebong RNNo ratings yet
- Saudi Prometric Latest Questions AndanswerDocument67 pagesSaudi Prometric Latest Questions AndanswerGloria Jaison100% (4)
- Formulation and Evaluation of Diclofenac Sodium Sustained Release Tablets Using Seed Powder of Strychnos potatorumDocument5 pagesFormulation and Evaluation of Diclofenac Sodium Sustained Release Tablets Using Seed Powder of Strychnos potatorumAreerietinqitink Onenkonenk TazqimaninaaNo ratings yet
- Mudravig PDFDocument24 pagesMudravig PDFJai KanthNo ratings yet
- Occupational Safety and Health Management: Prepared By: Puan Masliza MaskinDocument43 pagesOccupational Safety and Health Management: Prepared By: Puan Masliza MaskinAugustine JR RobertNo ratings yet
- Parental Alienation Is SERIOUS Child Abuse 2018 Wilfrid Von Boch-Galhau Parental Alienation Is in The DSMDocument15 pagesParental Alienation Is SERIOUS Child Abuse 2018 Wilfrid Von Boch-Galhau Parental Alienation Is in The DSML9at100% (6)
- Medical 1 PDFDocument5 pagesMedical 1 PDFsuresh balajiNo ratings yet
- Chapter1 Intro of Biomedical Signal ProcessingDocument50 pagesChapter1 Intro of Biomedical Signal ProcessingShafayet Uddin100% (3)
- It PDFDocument385 pagesIt PDFCosmina UngurNo ratings yet
- ECG Identification QuizDocument40 pagesECG Identification QuizRahul AudenesenNo ratings yet
- De Gruchys Clinical Haematology PDFDocument1 pageDe Gruchys Clinical Haematology PDFShivanshi K0% (1)
- MinoxidilDocument2 pagesMinoxidilHenna AhmedNo ratings yet
- Pediatric PulmonologyDocument250 pagesPediatric Pulmonologyshankargoudachildicu100% (4)
- Pulse Sequences: Application BrochureDocument184 pagesPulse Sequences: Application BrochureNguyễn CảnhNo ratings yet
- Clonus: Definition, Mechanism, Treatment: ReviewDocument8 pagesClonus: Definition, Mechanism, Treatment: ReviewLuqmanul HakimNo ratings yet
- Barthel IndexDocument2 pagesBarthel Indexgania100% (1)
- Kriya For Balancing The ChakrasDocument5 pagesKriya For Balancing The ChakrasFedra Fox Cubeddu100% (2)
- Combat Lifesaver Guide to One-Person Bag Valve Mask VentilationDocument1 pageCombat Lifesaver Guide to One-Person Bag Valve Mask VentilationSae TumNo ratings yet
- DPD ResumeDocument3 pagesDPD Resumeapi-272384986No ratings yet
- Human Blood CellsDocument3 pagesHuman Blood CellscsamarinaNo ratings yet
- 53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Document9 pages53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Dina AyupnNo ratings yet
- Nervous SystemDocument8 pagesNervous Systemfadedphotograph12340No ratings yet
- Pediatric Voice PresentationDocument16 pagesPediatric Voice Presentationapi-254429093No ratings yet
- Overdentures Improve Chewing Efficiency and Bone SupportDocument8 pagesOverdentures Improve Chewing Efficiency and Bone SupportMezo SalahNo ratings yet
- Medical Council of Inida Declaration Form 2010-2011for FacultyDocument9 pagesMedical Council of Inida Declaration Form 2010-2011for FacultydrtpkNo ratings yet
- Framingham Risk Score SaDocument8 pagesFramingham Risk Score Saapi-301624030No ratings yet
- Asymptomatic BacteriuriaDocument23 pagesAsymptomatic BacteriuriaSabita PaudelNo ratings yet
- Stress (Biology) : 1 Etymology and Historical UsageDocument19 pagesStress (Biology) : 1 Etymology and Historical UsageZiedTrikiNo ratings yet
- 4 Measurement and ComputationDocument6 pages4 Measurement and ComputationBernardMarkMateoNo ratings yet