You might also like
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsFrom EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsRating: 4.5 out of 5 stars4.5/5 (14)
- Özgür - Scrum TestDocument1 pageÖzgür - Scrum TestNameNo ratings yet
- Chain Ladder Excel CaritatDocument108 pagesChain Ladder Excel CaritatGael BernarNo ratings yet
- 2019 AudProb ARevenueCycleDocument8 pages2019 AudProb ARevenueCycleJhun0% (2)
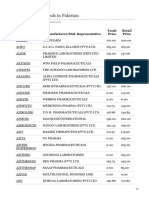
- Azithromycin Brands in Pakistan PDFDocument4 pagesAzithromycin Brands in Pakistan PDFibNo ratings yet
- PolicySoftCopy 5d46b6ba537a7b68d0636749Document5 pagesPolicySoftCopy 5d46b6ba537a7b68d0636749Vedashri1411No ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormAbhijeet SinhaNo ratings yet
- Easy Health Insurance Claim FormDocument8 pagesEasy Health Insurance Claim FormDiwakar NaiduNo ratings yet
- MediPrime Claim FormDocument8 pagesMediPrime Claim Formrahul0105100% (1)
- Claim Form Dhs ReimbursementDocument4 pagesClaim Form Dhs Reimbursementyyateen0% (1)
- 2 Claim Form A - Other Than PA and TravelDocument3 pages2 Claim Form A - Other Than PA and TravelEkta ChauhanNo ratings yet
- Ericsson Claim Form PDFDocument2 pagesEricsson Claim Form PDFlovingsayrus100% (1)
- 1.reimbursement Claim FormDocument3 pages1.reimbursement Claim FormVijiNo ratings yet
- Reimbursement Claim Form Insured PDFDocument2 pagesReimbursement Claim Form Insured PDFmadhavjindalNo ratings yet
- Claim Form - Part ADocument3 pagesClaim Form - Part Agrajesh45No ratings yet
- New Claim Form TTK TPADocument2 pagesNew Claim Form TTK TPAAbhijit SawantNo ratings yet
- Nic Claim FormDocument2 pagesNic Claim FormGopalKrishnaNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument4 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Auser4timepass6237No ratings yet
- Claimform BPage1 2 PDFDocument2 pagesClaimform BPage1 2 PDFusilainetNo ratings yet
- Claim Form - Part B HospitalDocument2 pagesClaim Form - Part B Hospitalgrajesh45No ratings yet
- Standard Claim Form HospitalDocument2 pagesStandard Claim Form Hospitalnpatel35No ratings yet
- Claim Form Part-BDocument2 pagesClaim Form Part-BnaveenashokNo ratings yet
- Family Floater Claim FormDocument4 pagesFamily Floater Claim FormSAMNo ratings yet
- Claim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Document4 pagesClaim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Boby GanaNo ratings yet
- Standard Claim Form InsuredDocument2 pagesStandard Claim Form InsuredknsaravanaNo ratings yet
- IRDA Reimbursement Claim Form - InsuredDocument2 pagesIRDA Reimbursement Claim Form - InsuredSoham BanerjeeNo ratings yet
- New Claim Form Dhs ReimbursementDocument4 pagesNew Claim Form Dhs Reimbursementamit_bisht2225% (4)
- Claim Form Dhs ReimbursementDocument4 pagesClaim Form Dhs ReimbursementrenjithkunnumpurathNo ratings yet
- Reimbursement Claim Form PDFDocument1 pageReimbursement Claim Form PDFNaresh KaushikNo ratings yet
- National Insurance Company LimitedDocument6 pagesNational Insurance Company LimitedSneha SinhaNo ratings yet
- Claim FormDocument4 pagesClaim Formdharani633No ratings yet
- National Insurance - ClaimFormDocument6 pagesNational Insurance - ClaimFormPallav GangeleNo ratings yet
- CL AIM FO RM FO R HE ALT H INS UR AN CE PO Lici ES OT HE R TH AN TR AV EL AN D PE RS ON AL AC CID EN T-PA RT A To Be Filled in by The InsuredDocument5 pagesCL AIM FO RM FO R HE ALT H INS UR AN CE PO Lici ES OT HE R TH AN TR AV EL AN D PE RS ON AL AC CID EN T-PA RT A To Be Filled in by The InsuredyatishvijayNo ratings yet
- Pre Auth FormDocument2 pagesPre Auth FormRajdeep AdhyaNo ratings yet
- Newindiaclaim Form A InsuredDocument2 pagesNewindiaclaim Form A Insuredkbl11794No ratings yet
- Pre Authorisation Form - New CashlessDocument2 pagesPre Authorisation Form - New CashlessMitraNo ratings yet
- Health India TPA - Pre Auth FormDocument5 pagesHealth India TPA - Pre Auth FormBOOKREADER_NOW100% (1)
- Pre Auth Form Revised PDFDocument5 pagesPre Auth Form Revised PDFNILESHNo ratings yet
- Axa Claim FormDocument2 pagesAxa Claim FormReem Mohamed El BarraniNo ratings yet
- Claim Form Final - LowDocument5 pagesClaim Form Final - LowDipti BhanjaNo ratings yet
- Test AxaDocument2 pagesTest AxaElmedina Berin HalilovićNo ratings yet
- AXA Reimbursement Form ALL enDocument2 pagesAXA Reimbursement Form ALL enReynard Delos SantosNo ratings yet
- Max Bupa Claim Form NewDocument9 pagesMax Bupa Claim Form NewViral ShuklaNo ratings yet
- MaxBupa Reimbursement Claim FormDocument10 pagesMaxBupa Reimbursement Claim FormAnonymous L77eD5uoNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- Easy Health: Claim FormDocument4 pagesEasy Health: Claim FormCrystal GarciaNo ratings yet
- MSEB - Claim - Form 2016 MahaGencoDocument2 pagesMSEB - Claim - Form 2016 MahaGencoAnonymous pKsr5vNo ratings yet
- 05 - Domiciliary Claim FormDocument2 pages05 - Domiciliary Claim FormSAI SRI VLOGSNo ratings yet
- MD India Forms & Policy DocumentDocument42 pagesMD India Forms & Policy DocumentYagantiGaneshRaghuveerNo ratings yet
- Medical Claim Reimbursement Form EnglishDocument2 pagesMedical Claim Reimbursement Form EnglishHananAhmedNo ratings yet
- Reliance Health Claim FormDocument4 pagesReliance Health Claim FormarijitnirmalNo ratings yet
- Health Suraksha Claim FormDocument2 pagesHealth Suraksha Claim FormAnna MalaiNo ratings yet
- Secure (Personal Accident Insurance Product) Claim FormDocument10 pagesSecure (Personal Accident Insurance Product) Claim Formmestry.om05No ratings yet
- Claim Form IHealthcareDocument6 pagesClaim Form IHealthcareHarish AdityaNo ratings yet
- OPD Claim FormDocument1 pageOPD Claim FormKhalid SayeedNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Claim Form: (For Reimbursement of Expenses)Document4 pagesClaim Form: (For Reimbursement of Expenses)Shankar NathNo ratings yet
- Ap Chief Minister'S Relief FundDocument6 pagesAp Chief Minister'S Relief Fundiqbal1439988100% (1)
- Part B - Aditya BirlaDocument4 pagesPart B - Aditya BirlaRainbow Multispeciality HospitalNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- A Guide to District Court Civil Forms in the State of HawaiiFrom EverandA Guide to District Court Civil Forms in the State of HawaiiNo ratings yet
- Cable Tray DetailsDocument2 pagesCable Tray Detailssomasreekanth4220% (1)
- CheckList atDocument2 pagesCheckList atsomasreekanth422No ratings yet
- Tariff Schedule For FY2018-19Document11 pagesTariff Schedule For FY2018-19somasreekanth422No ratings yet
- 9 Point Check List For Buying Agricultural Land in Telangana & AP - FactlyDocument6 pages9 Point Check List For Buying Agricultural Land in Telangana & AP - Factlysomasreekanth422No ratings yet
- Motor DatasheetDocument6 pagesMotor Datasheetsomasreekanth422100% (1)
- Transformer 408-3100-100v 5 OutputDocument9 pagesTransformer 408-3100-100v 5 Outputsomasreekanth422No ratings yet
- Gen Circuit BreakerDocument8 pagesGen Circuit Breakersomasreekanth422No ratings yet
- Power System Protective Relaying: Basic Concepts, Industrial-Grade Devices, and Communication MechanismsDocument35 pagesPower System Protective Relaying: Basic Concepts, Industrial-Grade Devices, and Communication MechanismsAnonymous hWRGcOe4X100% (1)
- APGENCO1Document3 pagesAPGENCO1Potti PradeepNo ratings yet
- Ge SCADADocument4 pagesGe SCADAsomasreekanth422No ratings yet
- ACCP 5000 Test 2 Review ClassDocument26 pagesACCP 5000 Test 2 Review ClassDang ThanhNo ratings yet
- HSBC Bank (Singapore) Limited HSBC Credit / Debit Card - Dispute Declaration FormDocument2 pagesHSBC Bank (Singapore) Limited HSBC Credit / Debit Card - Dispute Declaration FormYeong WheeNo ratings yet
- About AonDocument6 pagesAbout AonAmit ChauhanNo ratings yet
- Test 1Document1 pageTest 1SARESH STUDIONo ratings yet
- HW SD-WAN 03 Networking and PlanningDocument59 pagesHW SD-WAN 03 Networking and Planningxem phimNo ratings yet
- Cloud Academy Calendar July 2023 - Azure CloudDocument6 pagesCloud Academy Calendar July 2023 - Azure CloudAditi PandeyNo ratings yet
- Contoh INVOICEDocument2 pagesContoh INVOICEzananur547No ratings yet
- AMADEUS QUICK REFERENCE - 6pg PDFDocument6 pagesAMADEUS QUICK REFERENCE - 6pg PDFManish SinghNo ratings yet
- Chapter 6 PPT - ODocument26 pagesChapter 6 PPT - ONgọc YếnNo ratings yet
- I. Difference Between JLG and SHG Models of MicrofinanceDocument4 pagesI. Difference Between JLG and SHG Models of MicrofinanceSudip SahaNo ratings yet
- D 6109629839424099312Document11 pagesD 6109629839424099312status upadterNo ratings yet
- ? Thanks!Document6 pages? Thanks!NYAM CYRIL MUNANGNo ratings yet
- MortgageServicingBankAccountProgramMSP 2Document2 pagesMortgageServicingBankAccountProgramMSP 2Nye LavalleNo ratings yet
- M1 - Introduction To BFSIDocument14 pagesM1 - Introduction To BFSIGeorge BernardNo ratings yet
- Service Index PDF - PHP Content Id 2378053&content Tid 388906138&content Type TempDocument2 pagesService Index PDF - PHP Content Id 2378053&content Tid 388906138&content Type Tempshiripalsingh0167No ratings yet
- Form12BB R539 Proof Submission Form PDFDocument4 pagesForm12BB R539 Proof Submission Form PDFSiva ThotaNo ratings yet
- CS WCMC Assignment II AnsDocument8 pagesCS WCMC Assignment II AnsyeabmelkamuNo ratings yet
- Koothi PoondaDocument9 pagesKoothi Poondasasirkumar1No ratings yet
- Maayo Shipping Inc. Phase 3 PDFDocument74 pagesMaayo Shipping Inc. Phase 3 PDFIrish CabsNo ratings yet
- WCDMA OverviewDocument101 pagesWCDMA OverviewVarsanNo ratings yet
- Multiplexing and DemultiplexingDocument48 pagesMultiplexing and DemultiplexingAkpevwe IsireNo ratings yet
- Ins II Assignments PGDMFCDocument2 pagesIns II Assignments PGDMFCKumar MayankNo ratings yet
- Place of SupplyDocument6 pagesPlace of SupplyMadhuram SharmaNo ratings yet
- Rewards: A Thing Given in Recognition of One's Service, Effort, or AchievementDocument47 pagesRewards: A Thing Given in Recognition of One's Service, Effort, or AchievementmeeeeehhhNo ratings yet
- Air BNB 2017Document2 pagesAir BNB 2017GoMNNo ratings yet