You might also like
- Hkhomc4&Annotation - Id Annotation - 2671999901: 1. Haelo Uk. Patient Safety Briefing 1.1 - YoutubeDocument1 pageHkhomc4&Annotation - Id Annotation - 2671999901: 1. Haelo Uk. Patient Safety Briefing 1.1 - YoutubeDewi SekarsariNo ratings yet
- Liriklagu Some Soyou JunggigoDocument1 pageLiriklagu Some Soyou JunggigoWidya YusmaNo ratings yet
- Comparative Study of The Impact of Intoxication On Injuries in China and KoreaDocument7 pagesComparative Study of The Impact of Intoxication On Injuries in China and KoreaDewi SekarsariNo ratings yet
- Jurnal InternasionalDocument15 pagesJurnal InternasionalDewi SekarsariNo ratings yet
- Jurnal InternasionalDocument15 pagesJurnal InternasionalDewi SekarsariNo ratings yet
- The Asia-Pacific Journal: Japan Focus: In-Depth Critical Analysis of The Forces Shaping The Asia-Pacific... and The WorldDocument3 pagesThe Asia-Pacific Journal: Japan Focus: In-Depth Critical Analysis of The Forces Shaping The Asia-Pacific... and The WorldDewi SekarsariNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Frontliners HirarcDocument8 pagesFrontliners HirarcSitiAliahNo ratings yet
- DAFTAR PUSTAKA HydrocephalusDocument2 pagesDAFTAR PUSTAKA HydrocephalusRahma darisNo ratings yet
- Follicle-Stimulating Hormone: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Document4 pagesFollicle-Stimulating Hormone: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Jimboreanu György PaulaNo ratings yet
- HSE Lecture NotesDocument10 pagesHSE Lecture NotesAndreNo ratings yet
- MChiro Prospectus 2021Document22 pagesMChiro Prospectus 2021Aura-Elena BugusNo ratings yet
- 1548 6066 1 PBDocument10 pages1548 6066 1 PBOun VikrethNo ratings yet
- Physiological Responses To Lead Exposure in Wheat, Barley and OatDocument6 pagesPhysiological Responses To Lead Exposure in Wheat, Barley and OatVince RomanoNo ratings yet
- Yellow FeverDocument21 pagesYellow Fevernitu73No ratings yet
- Eco Tex - Google Search PDFDocument1 pageEco Tex - Google Search PDFAbdul RaheemNo ratings yet
- Quantitative Analysis of Miller Mobility Index For The Diag 2018 Journal ofDocument5 pagesQuantitative Analysis of Miller Mobility Index For The Diag 2018 Journal ofAgung AdhaNo ratings yet
- EpicondilteDocument7 pagesEpicondilteRicardo fariaNo ratings yet
- Theoretical Foundation of NursingDocument36 pagesTheoretical Foundation of NursingIsmael JaaniNo ratings yet
- NBDE Part 1 TipsDocument2 pagesNBDE Part 1 Tipsasda20148783% (6)
- Chapter - 3 Fibre To Fabric: 5.7.2021: Class - 7Document4 pagesChapter - 3 Fibre To Fabric: 5.7.2021: Class - 77A04Aditya MayankNo ratings yet
- Fire Your WifeDocument35 pagesFire Your Wifeonlineguy2449No ratings yet
- Mountain of Fire & Miracles Ministries: International Headquarters, Lagos. Prayer PointsDocument2 pagesMountain of Fire & Miracles Ministries: International Headquarters, Lagos. Prayer PointsMhedo Bolarinwa AkanniNo ratings yet
- QP-005 Training ProcessDocument3 pagesQP-005 Training Processesraa asemNo ratings yet
- Journal On Self ConceptDocument6 pagesJournal On Self Conceptkspsridharan4899No ratings yet
- Yashraj ResultDocument2 pagesYashraj ResultSom DevNo ratings yet
- Mary-Joan Gerson - The Embedded Self, Second Edition - An Integrative Psychodynamic and Systemic Perspective On Couples and Family Therapy (2009)Document304 pagesMary-Joan Gerson - The Embedded Self, Second Edition - An Integrative Psychodynamic and Systemic Perspective On Couples and Family Therapy (2009)India Represents100% (1)
- Push Jerk - CrossFit Training GuideDocument6 pagesPush Jerk - CrossFit Training GuideDominik KadlecNo ratings yet
- Child Psychology Psychiatry - 2020 - Lavis - Online Harms or Benefits An Ethnographic Analysis of The Positives andDocument13 pagesChild Psychology Psychiatry - 2020 - Lavis - Online Harms or Benefits An Ethnographic Analysis of The Positives andclaudyaNo ratings yet
- ResponsibleRestart Ohio: County FairsDocument2 pagesResponsibleRestart Ohio: County FairsTiffinOhio.netNo ratings yet
- Bioethics Session 16 SASDocument4 pagesBioethics Session 16 SASAnthony BadiliNo ratings yet
- Artikel Dita Nova SaputriDocument6 pagesArtikel Dita Nova SaputriDita Nova SaputriNo ratings yet
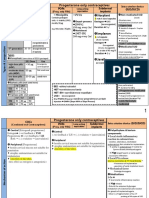
- Norplant: Progesterone Only ContraceptivesDocument9 pagesNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyNo ratings yet
- Decee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverDocument5 pagesDecee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverJeff Mac Rae RamosNo ratings yet
- Diabetes Research PaperDocument7 pagesDiabetes Research PaperLysol007100% (3)
- Đề thi TS NK Anh (chuyên) 18-19Document10 pagesĐề thi TS NK Anh (chuyên) 18-19Trung KiênNo ratings yet
- Case 1Document3 pagesCase 1Kenneth NovenoNo ratings yet