You might also like
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesFrom EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesNo ratings yet
- LMCC II GuideDocument79 pagesLMCC II GuideSoleil DaddouNo ratings yet
- Clinical Skills Review: Scenarios Based on Standardized PatientsFrom EverandClinical Skills Review: Scenarios Based on Standardized PatientsRating: 4 out of 5 stars4/5 (10)
- Essential Examination, third edition: Step-by-step guides to clinical examination scenarios with practical tips and key facts for OSCEsFrom EverandEssential Examination, third edition: Step-by-step guides to clinical examination scenarios with practical tips and key facts for OSCEsRating: 3 out of 5 stars3/5 (5)
- 99 Topics for the CCFP: A concise guide to family medicineDocument134 pages99 Topics for the CCFP: A concise guide to family medicinealexidr100% (2)
- CFPC SampsDocument39 pagesCFPC SampsSumer Chauhan100% (9)
- Guide To The Certification Examination in Family MedicineDocument29 pagesGuide To The Certification Examination in Family Medicineأحمد خيري التميميNo ratings yet
- Family MedicineDocument156 pagesFamily MedicinedtriggNo ratings yet
- Ocfp 2014 2015 Guidebook Final May 26 PDFDocument67 pagesOcfp 2014 2015 Guidebook Final May 26 PDFaayceeNo ratings yet
- Rational Laboratory and Diagnostic TestsDocument26 pagesRational Laboratory and Diagnostic TestsCeline dela cruzNo ratings yet
- Canadian Screening GuidelinesDocument8 pagesCanadian Screening GuidelinesaayceeNo ratings yet
- 101 Clinical Cases in Emergency Room Book PDFDocument1 page101 Clinical Cases in Emergency Room Book PDFHhaNo ratings yet
- MRCGP Oral Exam Sample Questions and Ethical FrameworkDocument21 pagesMRCGP Oral Exam Sample Questions and Ethical FrameworkSalah ElbadawyNo ratings yet
- FRCEM FINAL: Critical Appraisal Made Easy e-BookFrom EverandFRCEM FINAL: Critical Appraisal Made Easy e-BookRating: 5 out of 5 stars5/5 (1)
- Study Notes Emergency MedicineDocument12 pagesStudy Notes Emergency MedicineMedShare57% (7)
- Family Medicine - General Practice MEQ 2006Document6 pagesFamily Medicine - General Practice MEQ 2006jermie22100% (1)
- Family MedicineDocument42 pagesFamily Medicineakufahaba100% (5)
- Hot Topics for Cardiovascular DiseaseDocument13 pagesHot Topics for Cardiovascular Diseasegautambob29% (7)
- Family Medicine Guide for Common ConditionsDocument42 pagesFamily Medicine Guide for Common ConditionsRojelle LezamaNo ratings yet
- Passmedicine MRCP Notes-Palliative Medicine and End of Life CareDocument5 pagesPassmedicine MRCP Notes-Palliative Medicine and End of Life CareMayar WaelNo ratings yet
- AKT Feedback Jan 2017Document5 pagesAKT Feedback Jan 2017asyouallNo ratings yet
- 99 Topics - Family Medicine Priority Topics and Key FeaturesDocument104 pages99 Topics - Family Medicine Priority Topics and Key FeaturesRica RoraNo ratings yet
- Racgp GuideDocument28 pagesRacgp Guidemyat252100% (1)
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023From EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023No ratings yet
- A Brief Introduction to the Multi-Specialty Recruitment Assessment (MSRA)From EverandA Brief Introduction to the Multi-Specialty Recruitment Assessment (MSRA)Rating: 5 out of 5 stars5/5 (1)
- TDM Exam Study Resources PDFDocument5 pagesTDM Exam Study Resources PDFDrosler MedqsNo ratings yet
- Pocket Primary Care (Pocket Notebook... by Curtis ChongDocument7,312 pagesPocket Primary Care (Pocket Notebook... by Curtis ChongPaolo A. Cabeza Martinez10% (10)
- RACGP Handbook For GP 2017-20Document68 pagesRACGP Handbook For GP 2017-20M Razibul Islam RazonNo ratings yet
- Medical student's guide to ranking topicsDocument60 pagesMedical student's guide to ranking topicsMuntaha Javed100% (2)
- How To Do Good in Na ExamDocument2 pagesHow To Do Good in Na ExamsuaqaziNo ratings yet
- Casebook Book: Famil yDocument24 pagesCasebook Book: Famil ylentini@maltanet.net100% (1)
- PANCE (Physician Assistant Nat. Cert Exam) Flashcard BookFrom EverandPANCE (Physician Assistant Nat. Cert Exam) Flashcard BookRating: 1.5 out of 5 stars1.5/5 (4)
- MRCGP Int OsceDocument81 pagesMRCGP Int OsceAbdelnasir Abbas Abdalla ELsheikh100% (3)
- Emergency Medicine SummaryDocument4 pagesEmergency Medicine SummaryokibreazyNo ratings yet
- General Practice Collection GuideDocument2 pagesGeneral Practice Collection GuideAdrian HawordNo ratings yet
- Emergency Medicine Sample SampsDocument19 pagesEmergency Medicine Sample SampsH!TNo ratings yet
- Plab2 Stations Topics New Old PDFDocument6 pagesPlab2 Stations Topics New Old PDFBeaulahNo ratings yet
- GP 2012 Handbook - OnlineDocument27 pagesGP 2012 Handbook - OnlinejoobazhieNo ratings yet
- Family Medicine Exam Manual 2011Document72 pagesFamily Medicine Exam Manual 2011SultanAlam100% (1)
- U.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideFrom EverandU.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideNo ratings yet
- Emergency Department Design: A Practical Guide to Planning for the Future, 2nd EditionFrom EverandEmergency Department Design: A Practical Guide to Planning for the Future, 2nd EditionRating: 1 out of 5 stars1/5 (1)
- Urgent and Out-of-Hours Primary Care: A practical guide for cliniciansFrom EverandUrgent and Out-of-Hours Primary Care: A practical guide for cliniciansRating: 5 out of 5 stars5/5 (1)
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- Eureka: Clinical Skills, Diagnostics and ReasoningFrom EverandEureka: Clinical Skills, Diagnostics and ReasoningRating: 5 out of 5 stars5/5 (2)
- Emergency Medicine Cases: Case 1Document33 pagesEmergency Medicine Cases: Case 1skeebs23100% (1)
- Red Flags For The MRCGPDocument3 pagesRed Flags For The MRCGPUsm LeeNo ratings yet
- Csa - Rams Top Tips Part 1Document7 pagesCsa - Rams Top Tips Part 1Zaheer AliNo ratings yet
- Patrick Vallance - The Edmonton Manual - Approach To The OSCE (2019)Document500 pagesPatrick Vallance - The Edmonton Manual - Approach To The OSCE (2019)Tvisha50% (2)
- Simulated Clinic Tips and PitfallsDocument27 pagesSimulated Clinic Tips and PitfallsFayzaRayesNo ratings yet
- 10 - Toronto Notes 2011 - Family MedicineDocument54 pages10 - Toronto Notes 2011 - Family MedicineDeyaa Mansouri100% (1)
- IDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistDocument3 pagesIDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistStacey WoodsNo ratings yet
- Tamiflu PrescribingDocument26 pagesTamiflu PrescribingStacey WoodsNo ratings yet
- Id 397 TeicoplaninDocument2 pagesId 397 TeicoplaninStacey WoodsNo ratings yet
- Switching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilDocument2 pagesSwitching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilGlory Claudia KarundengNo ratings yet
- Antibiotic Selection - The Clinical AdvisorDocument6 pagesAntibiotic Selection - The Clinical AdvisorStacey WoodsNo ratings yet
- Appropriate Use of Laxatives in The Older PersonDocument7 pagesAppropriate Use of Laxatives in The Older PersonStacey WoodsNo ratings yet
- J Jacadv 2023 100389Document12 pagesJ Jacadv 2023 100389Edward ElBuenoNo ratings yet
- Management of Bacterial and Fungal Infections in Cirrhosis JOH 2021Document17 pagesManagement of Bacterial and Fungal Infections in Cirrhosis JOH 2021Francisco Javier Gonzalez NomeNo ratings yet
- Palliative2 Nausea MedtableDocument2 pagesPalliative2 Nausea MedtableStacey WoodsNo ratings yet
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocument2 pagesTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsNo ratings yet
- Antithrombotic Therapy For VTE DiseaseDocument13 pagesAntithrombotic Therapy For VTE DiseaseStacey WoodsNo ratings yet
- Multimorbidity Clinical Assessment and Management 1837516654789Document22 pagesMultimorbidity Clinical Assessment and Management 1837516654789Stacey WoodsNo ratings yet
- 2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitDocument19 pages2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitStacey WoodsNo ratings yet
- Critical CareDocument8 pagesCritical CareDzikrul Haq KarimullahNo ratings yet
- Splenectomy Guideline Final 2012Document6 pagesSplenectomy Guideline Final 2012Stacey WoodsNo ratings yet
- Antibiotik WhoDocument49 pagesAntibiotik WhodjebrutNo ratings yet
- C.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestDocument2 pagesC.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestStacey WoodsNo ratings yet
- Drug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseDocument6 pagesDrug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseStacey WoodsNo ratings yet
- Stimulant May Speed Antidepressant Response Time in ElderlyDocument3 pagesStimulant May Speed Antidepressant Response Time in ElderlyStacey WoodsNo ratings yet
- Biomarkers of SepsisDocument8 pagesBiomarkers of SepsisStacey WoodsNo ratings yet
- Procoagulant GuidelineDocument30 pagesProcoagulant GuidelineStacey WoodsNo ratings yet
- Antimicrobials at The End of LifeDocument2 pagesAntimicrobials at The End of LifeStacey WoodsNo ratings yet
- Potasio. 2014.Document19 pagesPotasio. 2014.Nestor Enrique Aguilar SotoNo ratings yet
- Preoperative Insulin 2013Document3 pagesPreoperative Insulin 2013Stacey WoodsNo ratings yet
- Fluid Choices Impact Outcome in Septic ShockDocument7 pagesFluid Choices Impact Outcome in Septic ShockStacey WoodsNo ratings yet
- StrokeDocument2 pagesStrokeStacey WoodsNo ratings yet
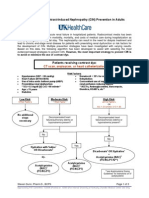
- Contrast NephRopathy GuidelinesDocument3 pagesContrast NephRopathy GuidelinesStacey WoodsNo ratings yet
- Airway Clearance in The Intensive Care UnitDocument5 pagesAirway Clearance in The Intensive Care UnitStacey WoodsNo ratings yet
- Elderly Patients Making Wise ChoicesDocument6 pagesElderly Patients Making Wise ChoicesStacey WoodsNo ratings yet
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamNo ratings yet
- Resolving Trauma With Bioenergetics: Niki GratrixDocument18 pagesResolving Trauma With Bioenergetics: Niki GratrixframistatNo ratings yet
- 500 Nursing QuestionsDocument209 pages500 Nursing QuestionsFilipino Nurses Central90% (20)
- Healing The Invisible WoundsDocument32 pagesHealing The Invisible WoundsShannon ColeNo ratings yet
- Orange County Court Corruption - ProTem - Judge Grainne Ward - BriceDocument29 pagesOrange County Court Corruption - ProTem - Judge Grainne Ward - Bricetheplatinumlife7364100% (1)
- Coping Styles and PersonalityDocument127 pagesCoping Styles and PersonalityJorge Pedro TresymedioNo ratings yet
- PATIENT COUNSEL - Palak RaiyaDocument18 pagesPATIENT COUNSEL - Palak RaiyaPalak RaiyaNo ratings yet
- PSY 315 TUTOR Principal EducationDocument43 pagesPSY 315 TUTOR Principal Educationtoshibamusic5No ratings yet
- Amygdala FunctionDocument5 pagesAmygdala FunctionRich Cole100% (1)
- Alain Brunet, Scott P. Orr, Jacques Tremblay, Kate Robertson, Karim Nader, Roger K. PitmanDocument4 pagesAlain Brunet, Scott P. Orr, Jacques Tremblay, Kate Robertson, Karim Nader, Roger K. PitmanNicole Baumgartner LoebNo ratings yet
- The Link Between Homelessness and Mental Illness (ABingham)Document18 pagesThe Link Between Homelessness and Mental Illness (ABingham)Adeleida BinghamNo ratings yet
- PTSD Checklist Civilian VersionDocument2 pagesPTSD Checklist Civilian VersionVVlynnNo ratings yet
- PCL S PDFDocument1 pagePCL S PDFspectre68No ratings yet
- Moviearticlenotes 2Document4 pagesMoviearticlenotes 2api-315916747No ratings yet
- 34 Jan 2011 PDFDocument136 pages34 Jan 2011 PDFNikita JoshiNo ratings yet
- Anxiety Disorder and Its TypesDocument32 pagesAnxiety Disorder and Its TypesWiwi Wulandani AbNo ratings yet
- MCQ, PMP & Essay Psychiatry CombinedDocument23 pagesMCQ, PMP & Essay Psychiatry CombinedAiman Arifin100% (1)
- Therapeutic Journaling BenefitsDocument6 pagesTherapeutic Journaling BenefitsAura SkyNo ratings yet
- His Brain Her Brain PDFDocument9 pagesHis Brain Her Brain PDFInterfan_allinNo ratings yet
- Neuropsychological RehabilitationDocument26 pagesNeuropsychological RehabilitationMaría Belén FaríasNo ratings yet
- Critical care patients' psychosocial problemsDocument5 pagesCritical care patients' psychosocial problemsSaif Ahmed jubarNo ratings yet
- Psychiatric Nursing Practice Test 6Document9 pagesPsychiatric Nursing Practice Test 6Filipino Nurses CentralNo ratings yet
- Climate Change and Mental Health: Psychosocial Disaster Efforts After Haiti Earthquake, Dr. Judy KurianskyDocument35 pagesClimate Change and Mental Health: Psychosocial Disaster Efforts After Haiti Earthquake, Dr. Judy KurianskyHere & NowNo ratings yet
- Therapeutic CommunicationDocument7 pagesTherapeutic CommunicationJoseph Rommel Castro CortezNo ratings yet
- NCAA ComplaintDocument64 pagesNCAA ComplaintAlex AbramiNo ratings yet
- Chronic Health Challenges ANSWER KeyDocument97 pagesChronic Health Challenges ANSWER KeyDol PhinNo ratings yet
- Write Science AbstractDocument5 pagesWrite Science AbstractAndi Muhammad IkhwanNo ratings yet
- The Body Keeps The ScoreDocument46 pagesThe Body Keeps The ScoreCatalina Ursa50% (4)
- Sim DRRM Melc Q1 Week 2 L4 5 - 24 PDFDocument24 pagesSim DRRM Melc Q1 Week 2 L4 5 - 24 PDFVital Mark ianNo ratings yet
- Assessment, Diagnosis and FormulationDocument30 pagesAssessment, Diagnosis and FormulationVani Jain100% (1)