DOI: 10.5958/2319-5886.2015.00020.
International Journal of Medical Research
&
Health Sciences
www.ijmrhs.com
Volume 4 Issue 1
th
Received: 6 Nov 2014
Research article
Coden: IJMRHS
Copyright @2014
ISSN: 2319-5886
th
Revised: 16 Dec 2014
Accepted: 25th Dec 2014
CLINICAL ISOLATES OF MECA, METHICILLIN, VANCOMYCIN RESISTANCE S. AUREUS; ESBLs
PRODUCING K.PNEUMONIA, E.COLI, P. AUREGENOSA FROM VARIOUS CLINICAL SOURCE
AND ITS ANTIMICROBIAL RESISTANCE PATTERNS
*Ismail Mahmud Ali1, Amirthalingam R2
1
Hospital Director, Head, Assistant Professor, Department of Surgery, Ibn Sina Teaching Hospital,
Specialist, Dept of Molecular biology, Ibn Sina Teaching Hospital, Sirt University, Libya, P.O. Box 705
*Corresponding author email: amrithrgenes@yahoo.co.in
ABSTRACT
Background and Objective: Antimicrobial resistance has turned into a key medical and public health crisis
globally since the injudicious use of magic bullets (drugs). Aim of this study is focused on the clinical isolate and
their percentages of resistant to antibiotics in gram positive bacteria such as MRSA, VRSA, and MSSA are
common causes of nosocomical, skin structure infections, bacteremia and infection of other systems; ESBLs
producing Enterobacteriaceae (E. coli, Klebsiella spp.) is common agent of urinary tract, bloodstream, pulmonary
and intra-abdominal infections and carbapenem resistant P. aeruginosa with its complete antimicrobial patterns
which are currently practiced in this population. Methods: There are one hundred and fourteen (114) various
clinical isolates, isolated from various clinical samples like throat swab, urine, pus, sputum, and blood culture,
identified as specific isolate with resistance patterns were analyzed by BD phoenix-100 the auto analyzer.
Results: Off 114 clinical isolate, 6 mecA-mediated resistance (cefoxitin>8mgc/ml), 11 methicillin resistance, 18
lactam/lactamase inhibitor, 12 methicillin sensitive and 3 vancomycin (>16g/ml) resistance S. aureus have
been isolated from overall 50 isolate of S.aureus. In addition, there are 27 P.aeruginosa, 15 ESBLs from overall
of 25 K. pneumoniae and 7 ESBLs out of 12 Escherichia coli species have been isolated. The resistance and
susceptibility pattern percentages have been graphically represented for each isolates. Conclusion: Current study
revealed that the drug classes of lactam/lactamase inhibitor having high resistance rate with S.aureus,
P.aureginosa, K. pneumoniae and E. coli isolate. Also, some of other drug classes such as cepham and
tetracycline having higher resistance rate with P.aureginosa and K.pneumoniae. In addition, the vancomycin
resistances S. aureus have been isolated and reported as first time in this population.
Keywords: Methicillin & Vancomycin Resistance, Methicillin Sensitive Staphylococcus aureus; extended
spectrum lactamases (ESBLs).
INTRODUCTION
A number of bacterial infections are caused by gram
negative aerobic and facultative anaerobic bacteria, it
belongs to the family of Enterobacteriaceae and nonEnterobacteriaceae. The gram positive bacteria
belong to the genera Staphylococcus, Enterococcus,
gram positive cocci and gram positive bacilli, all of
them are causative agents of nosocomial and
Ismail et al.,
community acquired infectious diseases in human
habitual life. Nearly 10 million children under the age
of 5 years have been died until the period of 2008 and
this effect enhanced the socioeconomic condition in
many developing countries, better management in
infection control, fast access immunization and
introduction of new vaccines against bacterial
123
Int J Med Res Health Sci. 2015;4(1):123-129
infection diseases1-2. The aerobic and facultative
anaerobic gram negative bacterium such as K.
pneumoniae, E. coli and P. aeruginosa, and gram
positive bacteria like S. aureus are multi-drugs
resistance bacterium and currently it is very common
in this local population as well as Ibn Sina Teaching
Hospital setup. This antimicrobial resistance is a
natural biological phenomenon and it is operated by a
genetic material (Nucleic acid) of living microbes
such as plasmids, transposons and integrons, it has
major roles in extension of multi-drugs resistance in
all bacterium3. Staphylococcus aureus is an
opportunistic hospital associated (HA-MRSA) and
community associated (CA-MSSA) infectious
bacterium in human body. The one called methicillin
resistant Staphylococcus aureus (MRSA) contain a
mecA gene that makes resistance to all -lactam
antibiotics including penicillin and cephalosporin;
methicillin sensitive Staphylococcus aureus (MSSA)
susceptible to many antibiotics other than lactam,
and vancomycin resistance S. aureus (VRSA)
resistant to long time use of glycopeptides antibiotics.
It can cause soft tissue infection as well as
pneumonia,
endocarditic,
septic
arthritis,
osteomyelitis, meningitis and septicemia. Hence,
Hospital acquired MRSA isolates are major causes of
nosocomial infections. The community associated
MRSA strains are significantly associated with soft
tissue infection, it also causes sepsis, necrotizing
fasciitis, and necrotizing pneumonia. It is an epidemic
as well as endemic all over the world4. Extended
spectrum lactamases (ESBLs) are enzymes
produced by different types of Enterobacteriaceae
family including Klebsiella pneumonia, E. coli, and
non-fermentative gram negative bacteria, such as
Pseudomonas
aeruginosa
and
Acinetobacter
baumannii. It is derived from (Temoniera patients)
TEM or sulphydroxyl variable (SHV) enzymes (for
resistance of ceftazidime and ceftriaxone antibiotic)
types of plasmid mediated lactamases through gene
mutation (amino acid alteration). The CTX-M type
enzymes are replacing SHV and TEM types
enzymes in nosocomial and community acquired
infections caused by E. coli and K. pneumoniae5. The
K, pneumoniae carbapenemase (KPC) is an enzyme
of K, pneumoniae for resisting multi-drugs like
lactams, fluoroquinolones, and amino glycosides drug
classes. These types of KPC infection may cause high
therapeutic failure with 50% of mortality rates6-7.
Ismail et al.,
Current study mainly focused on the isolation of
resistant and multi-drugs resistant pathogenic
bacterium and its antimicrobial susceptibility
patterns. The ultimate goal of this study is to guide
the health care workers and specialists to manage
such type of infections in an ethical and scientific
way and also guide for the society of infectious
disease panel and Ministry of Health in Libya.
MATERIALS AND METHODS
Clinical Samples: In the prospective analysis, a total
of 114 different bacterial isolates have been identified
from different clinical sources. The clinical sources
were sputum, urine, pus, wound & throat swabs, and
blood culture, received from Ibn Sina Teaching
Hospital and Out Patients during the years of 20132014. Although, some of exist datas during the years
of 2008 were integrated in this research for
highlighting the vancomycin resistance S.aureus have
been isolated previously by BD expert in this locality.
The dose of each drugs have been mentioned in all
graphs, because of the drugs concentration were
differed in each pathogenic bacterium so please refer
to the graphs. The drugs classes were included for all
clinical
isolate
such
as
5-fluoroquinolone
(Ciprofloxacin-CIP,
Norfloxacin-NOR,
Levofloxacin-LUX, Moxifloxacin-MXF) ; Amino
glycoside (Gentamicin-GM, Amikacin-AN);
lactam/beta-lactamase Inhibitor (Ampicillin AM,
Penicillin-G,-P,Oxacillin-OX,
Amoxicillin/
Clavulanate-AMC, Piperacillin-PIP); Carbapenam
(Imipenem-IPM,
Meropenem-MEM);
Folate
Antagonist (Trimethoprim/ Sulfamethoxazole-SXT);
Glycopeptides (Vancomycin-VA); Cephem (
Cephalothin-CF,Cefuroxime-CXM,CefoxitinFOX,Ceftazidine-CAZ,Cefotaxime-CTX, CefepimeCEP,
Ceftriaxone-CRO);
Lincosamide
(CCClindamycin);
Macrolide
(E-Erythromycin);
Nitro(FM-Nitrofurantion) ; Oxazolidine (LZDLinezolid) and Tetracycline. These are drugs names
with drugs classes have been applied according to the
gram stains concerns and rest of drugs classes have
been considered as exclusion criteria. The ethics
panel and internal review board of the organization
approved the procedure.
Culture Media preparation: There are some routine
mediums such as mac-conkey agar, nutrient agar,
blood agar (rest of clinical source and sensitivity),
chocolate agar (CSF), CLED agar for urine sample
124
Int J Med Res Health Sci. 2015;4(1):123-129
(Cystine-Lactose-Electrolyte-Deficient) and blood
culture bottle Bactech for blood samples (aerobic &
an-aerobic) were been used in the department of
clinical microbiology laboratory. These are all
powdered form except blood culture bottle and it has
been diluted according to the manufacturers
guidelines in the individual conical flask and further
autoclaved at 125 psi for 30 minutes, then it has been
cooled to room temperature and dispensed the liquid
substance with slightly lukewarm condition on
culture plates. Day by day the samples were received;
cultured, isolated, gram stained and applied as diluted
samples to the auto-microbial analyzer for further
confirmatory reasons. Hence, the culture medias are
recommended by manufacture to use in ID and AST
(antimicrobial susceptibility test) broth in system
analysis such as trypticase soy agar with 5% sheep
blood, bromthymol blue (BTB) lactose agar, BBLTM
chromagar TM orientation; chocolate agar; columbia
agar with 5% horse blood; columbia agar with 5%
sheep blood; cystine-lactose-electrolyte-deficient agar
(CLED); dey/engley (D/E) neutralizing agar; eosin
methylene blue; hektoen enteric agar; macconkey
agar; trypticase soy agar without blood; trypticase soy
agar with lecithin and tween 80 and xylose lysine
desoxycholate agar. Hence, dey/engley (D/E),
neutralizing agar; hektoen enteric agar; trypticase soy
agar without blood; trypticase soy agar with lecithin
and tween 80 and xylose lysine desoxycholate agar
are not recommended to use for AST broth in the
system analysis.
Bacterial Culture Isolation: The Major clinical
isolate have been confirmed with gram stains to get
verification of weather gram positive or negative
bacterium. After that, the clinical isolate have been
specified the bacteria, biochemical tests, and its
multi-drug susceptibility tests were performed
through BD-Phoenix-100, the microbial auto
analyzer.
BD Phoenix Panel: There are three more BD
phoenix panel kits have been introduced by
manufacturer to screen bacterial pathogens and each
panel has its own specific pathogenic identification
with drugs sensitivity and resistance patterns. Such as
PMIC/ID-69, PMIC and PID panels (Gram positive
pathogenic), NMIC/ID-94, NMIC and NID panels
(Gram negative pathogenic organisms) and special
panels only for SMIC/ID-11 panels (Streptococcus
species). The system can perform at least100 bacterial
identification with antimicrobial susceptibility at a
time. It utilizes an optimized colorimetric redox
indicator for AST, and a diversity of colorimetric and
fluorometric indicators for ID. The AST broth is cat
ion (Ca++ and Mg++) adjusted to optimize
susceptibility testing performance8.
Bacterial Identification: The ID portion of the
Phoenix panel utilizes a series of conventional,
chromogenic, and fluorogenic biochemical tests to
determine the identification of the organisms. The ID
broth contains 45 wells with dried biochemicals
substrate and two fluorescent control wells. Both
growth-based and enzymatic substrates are employed
to cover the different types of reactivity in the range
of taxa. The tests are based on microbial utilization
and degradation of specific substrates detected by
various indicator systems. Acid production is
indicated by a change in the phenol red indicator
when an isolate is able to utilize a carbohydrate
substrate. The chromogenic substrates produce a
yellow color upon enzymatic hydrolysis of either pnitro phenyl or p-nitroanilide compounds. Enzymatic
hydrolysis of fluorogenic substrates results in the
release of a fluorescent coumarin derivative.
Organisms that utilize a specific carbon source reduce
the resazurin-based indicator. In addition, there are
other tests that detect the ability of an organism to
hydrolyze, degrade, reduce, or otherwise utilize a
substrate9-10.
Antimicrobial Susceptibility Testing: The BD
Phoenix AST method is a broth based micro dilution
test. It contains 84 wells with dried antimicrobial
agents and one growth control well. The Phoenix
system utilizes a redox indicator for the detection of
organisms growth in the presence of an antimicrobial
agent. Continuous quantification of changes to the
indicator as well as bacterial turbidity is used in the
determination of bacterial growth. Each AST panel
configuration contains several antimicrobial agents
with a range of two fold doubling dilution
concentrations. Organism identification is used in the
interpretation of (the lowest concentration of an
antimicrobial agents in which no visible growth occur
is called minimal inhibitory concentration) MIC
values of each antimicrobial agent producing
Susceptible, Intermediate, or Resistant (SIR) result
classifications11.
BD Phoenix-100 Methods: BD Phoenix is an
automated microbiology system utilized for
125
Ismail et al.,
Int J Med Res Health Sci. 2015;4(1):123-129
recognition of pathogenic bacteria from pure culture
of different clinical samples. The pathogenic
organisms include the species of Staphylococcus,
Enterococcus, Gram positive bacilli and cocci, Gram
negative aerobic and facultative anaerobic bacteria
the family of Enterobacteriaceae and nonEnteterobacteriaceae. Also, it is future for in vitro
quantitative
determination
of
antimicrobial
susceptibility by minimal inhibitory concentration
(MIC).
The pure culture isolates have been tested with a
gram stain to assure the appropriate selection of
Phoenix panel type. Using aseptic technique, bacterial
colonies were picked from culture plate by sterile
swab and suspend the colonies into 4.5 ml of ID
broth. The BD Phoenix Spec Nephlometer has been
used to make inoculums densities purposes. There are
two types of inoculums density have been applied
(0.25 &0.5McFarland) for the panel type being run,
and then it ranges of 0.20 -0.30 to 0.50-0.60 was
acceptable. If the density of organisms is low then it
needs addition of bacterial colonies. Later on one
drop of AST indicator solutions was added to AST
broth solution (8.0ml); then 25l or 50l of bacterial
suspension were transferred from the ID tube into
AST broth tube according to the density of
suspension. These panels have been loaded into the
Phoenix instrument and continuously incubated at
35C until 16 hrs for the results gaining. There are
three different antibiotic methods (PMIC, NMIC and
SMIC) were been utilized in BD Phoenix-100 system
and the results were been reported as 95%
confidence automatically according to the
biochemical reaction the report have been released
with pathogenic names. Statistical analysis was done
by using micro software excel 2007.
RESULTS
There are 50 different types of S. aureus have been
isolated from various clinical samples with different
drug resistance patterns. Among fifty isolate, 6 mecA
mediated
resistant
staphylococcus
(MIC=
cefoxitin>8mcg/ml), 11methicillin (resistance of
ampicillin,
pencillin,
oxacillin
and
amoxicillin/clavulanate), 18 lactamase producing
staphylococcus aureus (susceptible to oxacillin and
amoxicillin), 12 methicillin sensitive (ampicillin,
oxacillin and amoxicillin/clavulanate) 3 vancomycin
(>16g/ml) resistance S.aureus and some of
heterogeneous vancomycin intermediate isolate have
been differentiated through auto analyzer from
various clinical samples .The selective antibiotic
usages have been graphically explained as
percentages with susceptible and resistance patterns
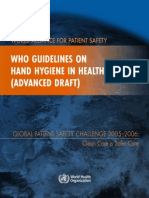
for S.aureus (refer to Fig-1). The most drug resistance
such as ampicillin (94%), penicillin (100%), oxacillin
(70%) and amoxicillin/clavulanate have been
observed as high resistance radio in among isolate of
S .aureus. The methicillin resistances S.aureus are
reported as high resistance to penicillin, lactam/lactamase inhibitor combinations, cephalosporins
and carbapenem because of ineffectiveness in clinical
usage but in this study carbapenem (imipenem 56%
and meropenem66%) is susceptible for S.aureus.
Fig 1: Antimicrobial resistance patterns for
S.aureus
Non-fermentative isolate such as Pseudomonas
aeruginosa is most frequently isolated as multidrug
resistance gram negative bacilli in routine clinical
microbiology laboratory. In current analysis, there are
twenty seven selective isolate have been isolated
from different clinical sources. The multidrug
resistance patterns have been observed as high in
lactam/ lactamase inhibitor (96-100%), folate
antagonist (100%), cephem (96-100%), and
tetracycline (100%). Hence, the moderate resistance
patterns also observed in 5-fluoroquinolone, amino
glycoside and carbapenem (Fig-2). Generally,
P.aeruginosa is intrinsically resistant to tetracycline;
primary quinolones, first generation and second
generation cephalosporin, amino penicillin/betalactamase inhibitor combinations, ertapenem,
ceftizoxime,
cefotaxime,
ceftriaxone,
chloramphenicol,
trimethoprim,
trimethoprim/
sulfamethoxazole and kanamycin were been
126
Ismail et al.,
Int J Med Res Health Sci. 2015;4(1):123-129
mentioned by BD expert. P.aeruginosa may develop
resistance during prolonged antimicrobial therapy
with all antibiotics. Norfloxacin and Tetracycline are
drugs of choice for urinary tract infection.
susceptibility rate was high in carbapenem than other
drug classes (Fig-4).
Fig 4: Antimicrobial resistance patterns for E.coli
Fig 2: Multidrug resistance patterns for
P.aeruginosa
Enterobacteriaceae family, mainly Klebsiella
pneumoniae and Escherichia coli are producing
lactam/ lactamase enzymes are able to deactivate the
antibiotic like lactam/lactamase drugs classes and it
also found in Pseudomonas aeruginosa. The current
analysis revealed that, more than 25 isolates from
different clinical samples such as sputum, urine, pus,
and throat swab. The resistance patterns of Klebsiella
pneumoniae have been graphically explained (Fig3).The highest resistance patterns were observed in
lactam/ lactamase and 5-fluoroquinolone drug
classes. The highest susceptibility prevalence was
observed in the drug class of carbapenem (88%).
Fig 3: Multidrug resistance patterns for
K.pneumoniae sp
Finally, the extended spectrum lactamase producing
E. coli isolate were observed among twelve isolates.
The highest drug resistance patterns were observed in
lactamase and tetracycline drugs classes and
Ismail et al.,
DISCUSSION
Resistance to antimicrobial drugs is a major health
crisis in Libya like others developing nations because
of lack of antimicrobial resistance survey and
improper management of drugs. Generally,
Staphylococcus aureus is well recognized as
causative agent of hospital-and community acquired
infections in this locality and it was first isolated as
MRSA in Benghazi in the year of 1972 by Goda12.
Later on it was reported in different Cities13, 14, 15.
Also, vancomycin resistance (MIC 16g/mL),
intermediate (4-8g/mL) and heterogeneous (14g/mL) S. aureus have been reported in US, Europe,
and Asia 16-17.However, there is no VRSA, VISA and
hVISA cases were reported in Libya by using
standard CLSI methods until 2011. Whereas in
present study, MRSA, MSSA, ESBLs producer and
vancomycin resistance S. aureus (MIC 16g/mL)
have been isolated and in brief high lightened with
resistance patterns in results division. Hence, some of
isolates were found with vancomycin sensitive,
heterogeneous and intermediate S. aureus.
Enterobacteriaceae
spp
mainly
Klebsiella
pneumoniae and E. coli bacterium are gram negative
bacterium. The K. pneumoniae OXA-48 producing
strains have been reported mainly from North African
countries, the Middle East, Turkey, India and other
European countries18-19. This bacterium steadily in
advance to resistance against -lactam antibiotics like
penicillin and cephalosporin by the assembling of
extended-spectrum lactamases (ESBLs) or
carbapenem-hydrolyzing enzymes for K. pneumoniae
20
. The another mobile metallo -lactamases enzymes
127
Int J Med Res Health Sci. 2015;4(1):123-129
produced by Pseudomonas aeruginosa spp in the
course of multidrug resistance activity and this type
of enzymes synthesis could be assorted from nation to
nation 21. Previous study of E.coli drugs resistance
pattern have been reported from Sirt, Tripoli and
Benghazi, during the years of 2002-2008.The
resistance pattern were ampcillin (49%,59%,57%);
chloramphenicol
(23%,21%,14%);
gentamicin
(9%,10%,7%); nalidixic acid (28%,28%,23%);
ciprofloxacin (2%,14%,17%) and trimethoprimsulfamethoxazole (36%,24%, 31%).22,23,24. Similarly,
the K. Pneumonia isolates proved to be resistant to all
broad-spectrum
cephalosporin
and
to
fluoroquinolones and susceptible to tigecycline were
reported from Italy during the Libyan conflict25.
Regarding resistance pattern in present study
(K.pneumonia & E.coli) were differed slightly from
previous report and should target more scientific
research on carbapenem and metallo -lactamases
producing isolates by molecular analysis in this
locality in feature.
The antibiotic resistance pattern in developing
countries like Iran, nearly 33% of ESBLs producing
K. pneumoniae causing major curative troubles and it
resistant was to ciprofloxacin and amino glycosides26;
though in India ESBL isolate drugs resistance were
amoxicillin (93.3%), gentamicin (70%), ciprofloxacin
(10.4%) and amikacin (26.1%)27. Likewise in present
study, lactam/lactamase drug class having high
resistance followed by cepham drug class for
K.pneumoniae and susceptibility ranges was higher in
carbaphenem drugs class. But in E .coli, lactam/
lactamase drugs class having high resistance followed
by tetracycline drug class and it susceptibility pattern
were 5- fluoroquinolone aminoglycoside and
carbapenem drugs class than nitrofurantoin and
cephem drugs class. The superior antimicrobial
resistance rates in current study could be attributed to
the resource of the clinical isolates being from
multispecialty setup and recurrent usage of broad
spectrum antibiotic. Also study might be helpful to
control of infectious diseases in public as well as poor
setup of hospitality.
CONCLUSION
Present study highlighted that the drug classes of
lactam/lactamase inhibitor having a high resistance
rate with S. aureus, P.aureginosa, K. pneumoniae and
E. coli isolate. Hence, some of other drugs classes
such as cepham and tetracycline also having higher
resistance rate with P.aureginosa and K.pneumoniae.
In addition, the vancomycin resistances S. aureus
have been isolated first time in this region by BD
phoenix expert and the clinical specialists should
concentrate much more in these cases. As a result,
superior antibiotic policy and hospital infection
management assessment can be making the first
move to prevent the emergence of multidrug resistant
clinical isolates.
ACKNOWLEDGEMENT: We would like to
convey our honest gratitude to microbiology teams.
Conflict of interest: None
REFERENCES
1. The State of the Worlds Children UNICEF 2007;
2008 http://www.unicef.org/ publications
2. Andre FE, Booy R, Bock HL, Clemens J, Datta
SK, John TJ. Vaccination greatly reduces disease,
disability, death and inequity worldwide. Bull
World Health Organ. 2008; 86:14046.
3. Dessen A, Di Guilmi AM, Vernet T, and
Dideberg O. Molecular mechanisms of antibiotic
resistance in gram-positive pathogens. Curr Drug
Targets Infect Dis. 2001;1:63-77.
4. Susan J, Rehm, Alan Tics. Staphylococcus
aureus: Methicillin-Susceptible S. aureus to
Methicillin-Resistant S .aureus and Vancomycin
resistant S. aureus. J.CID. 2010; 51(S2): S17682.
5. Jacoby GA, Munoz-Price LS. The new beta
lactamase. N. Engl J Med. 2005; 352:380-91.
6. Nordmann P, Cuzon G, Naas T. The real threat of
KPC carbapenemase-producing bacteria. Lancet
Infect Dis. 2009; 9: 228-36
7. Bradford PA, Bratu S, Urban C, Visalli M,
Mariano N, and Landman D. Emergence of
carbapenem
resistant
Klebsiella
species
possessing the class A carbapenem-hydrolyzing
KPC2 and inhibitor resistant TEM-30
lactamases in New York City. Clin Infect
Dis.2004; 39: 55-60.
8. Marymont JH, Wentz RM.Serial Dilution
Antibiotic Sensitivity Testing with the
Microtitrator
System.
Am.J.Clin-Pathol.
1966;45:548-51.
9. Kamper P, Rauhoff O, Dott W. Glycosidase
profiles
of
members
of
the
family
128
Ismail et al.,
Int J Med Res Health Sci. 2015;4(1):123-129
10.
11.
12.
13.
14.
15.
16.
17.
18.
Enterobacteriaceae.J.Clin.Microbiol.1991;29:287
7-79.
Manafi M, Kheifel W, Bascomb S.Fluorogenic
and Chromogenic Substrate used in Bacterial
Diagnosis. Microbial.Rev.1991.55: 335-348.
CLSI-M7-A6
Methods
for
Dilution
Antimicrobial Susceptibility Tests for Bacteria
that grow aerobically; Approved Standard-6th
Edition, January, 2003.
Goda
FFM.
Antibiotic
sensitivity
of
Staphylococcus aureus isolated from mastitis in
cows at Benghazi localities. Bull Animal Health
Product Africa.1976; 24: 47-52.
Zorgani A, Elahmer O, Franka E,Grera A,
Abudher A, Ghenghesh KS. Detection of
methicillin resistance Staphylococcus aureus
among healthcare workers in Libyan hospital. J
Hosp Infect.2009; 73: 91-2.
Belgasim Z, Saadaoui A, Zorgani A. Screening
for methicillin-resistant Staphylococcus aureus
among health care workers in the African
Oncology Institute, Sabrata- Libya. Am J Infect
Control.2010;38:498-9
Buzaid N, Elzouki A-N,Taher I, Ghenghesh KS.
Methicillin-resistance Staphylococcus aureus
(MRSA) in a tertiary surgical and trauma hospital
in Benghazi, Libya. J Infect Developing
Countries. 2011; 5: 2617-21s
Appelbaum
PC.
Reduced
glycopeptides
susceptibility
in
methicillin
resistance
Staphylococcus aureus (MRSA). Int J
Antimicrob Agents 2007; 30: 398-408.
Hageman JC, Patel J, Carey R, Tenover FC, and
McDonald LC,2009 accessed 30th October.
Investigation and control of vancomycinintermediate and resistance Staphylococcus
aureus: a guide for health departments and
infection
control
personnel
http://www.cdc.gov/ncidod/dhqp/pdf/ar/visavrsa-guide.pdf.
Nordmann P, Naas T, Poirel L. Global spread of
carbapenemase producing Enterobacteriaceae.
Emerg Infect Dis 2011; 17: 1791-1798.
19. Poirel L, Bonnin RA, Nordmann P. Genetic
features of the widespread plasmid coding for the
carbapenemase OXA-48.Antimicrob Agents
Chemother.2012;56:559-562.
20. Harris AD, Perencevich EN, Johnson JK,
Paterson DL, Morris JG, and Strauss SM et al.
Patient to patient transmission is important in
extended spectrum beta-lactamase producing
Klebsiella pneumoniae acquisition. Clin. Infect.
Dis.2007; 45: 134750.
21. Poirel
L,
Pitout
JD,
Nordmann
P.
Carbapenemases: Molecular diversity and clinical
consequences. Future Microbiology.2007; 2: 50112
22. Bgar SR, Hussein AA,Elahwel AM,Alani
SMH.Antibiotic resistance pattern of urinary tract
isolates. Jamahiriya Med J.2007; 7:116-21
23. Ghenghesh KS,Elkateb E,Berbash N, Nada RA,
Ahmed SF,and Rahouma A et al. Uropathogens
from diabetic patients in Libya: virulence factors
and phylogenetics groups of isolated E.coli. J
Med Microbiol. 2009; 58: 1006-14.
24. Buzayan MM, Tobgi RS,,Taher I. Detection of
extended spectrum -lactamases among urinary
E.coli and K.pneumoniae from two centers.
Jamahiriya Med J.2010;10: 10-6.
25. Kocsis E, Savio C, Piccoli M, Cornaglia G, and
Mazzariol A
et al. Klebsiella pneumonia
harbouring OXA-48 carbapenemase in a Libyan
refugee in Italy. Clin MicrobiolInfect.2013; 19:
E409-E411.
26. Liu SY, Su LH, Yeh YL, Chu C, Lai JC, and
Chiu CH. Characterization of Plasmids encoding
CTX-M-3extended-spectrum
beta-lactamase
from Enterobacteriaceae Isolated at a university
hospital in Taiwan. Int J Antimicrob Agents.
2007; 29, 440445.
27. Shukla I, Tiwari R, and Agrawal M. Prevalence
of extended spectrum lactamase producing
Klebsiella pneumoniae in a tertiary care hospital.
Indian J. Med. Microbiol. 2004; 22(1):8791.
129
Ismail et al.,
Int J Med Res Health Sci. 2015;4(1):123-129
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Grabovoi Numbers 2 PDF FreeDocument21 pagesGrabovoi Numbers 2 PDF FreeLina AmorNo ratings yet
- OMIC 311 Lecture 17 Human Papilloma, Herpes, Hepatits VirusDocument51 pagesOMIC 311 Lecture 17 Human Papilloma, Herpes, Hepatits VirusMaryam XANo ratings yet
- Hold Harmless AgreementDocument2 pagesHold Harmless Agreementapi-214452058No ratings yet
- Marketing Style Guide 1Document11 pagesMarketing Style Guide 1api-438812931No ratings yet
- Bawasig Pediatric ExamDocument20 pagesBawasig Pediatric Examخلدون سليمNo ratings yet
- Diagnosis of Honey Bee Diseases: United States Department of AgricultureDocument63 pagesDiagnosis of Honey Bee Diseases: United States Department of AgricultureBre ErbNo ratings yet
- OET Reading Test 5 - Part ADocument5 pagesOET Reading Test 5 - Part ALOTSOFTESTS91% (11)
- Ijmrhs Vol 4 Issue 4Document193 pagesIjmrhs Vol 4 Issue 4editorijmrhs0% (1)
- Ijmrhs Vol 4 Issue 3Document263 pagesIjmrhs Vol 4 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 1Document228 pagesIjmrhs Vol 3 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 2Document197 pagesIjmrhs Vol 2 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 4Document294 pagesIjmrhs Vol 3 Issue 4editorijmrhsNo ratings yet
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 3Document271 pagesIjmrhs Vol 3 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 4 Issue 2Document219 pagesIjmrhs Vol 4 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 2Document281 pagesIjmrhs Vol 3 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 3Document399 pagesIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- Ijmrhs Vol 2 Issue 4Document321 pagesIjmrhs Vol 2 Issue 4editorijmrhsNo ratings yet
- 48 MakrandDocument2 pages48 MakrandeditorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 1Document110 pagesIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- 45mohit EtalDocument4 pages45mohit EtaleditorijmrhsNo ratings yet
- Recurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoDocument2 pagesRecurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoeditorijmrhsNo ratings yet
- 47serban Turliuc EtalDocument4 pages47serban Turliuc EtaleditorijmrhsNo ratings yet
- 43chaitali EtalDocument3 pages43chaitali EtaleditorijmrhsNo ratings yet
- Williams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdultDocument3 pagesWilliams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdulteditorijmrhsNo ratings yet
- 38vaishnavi EtalDocument3 pages38vaishnavi EtaleditorijmrhsNo ratings yet
- 41anurag EtalDocument2 pages41anurag EtaleditorijmrhsNo ratings yet
- 35krishnasamy EtalDocument1 page35krishnasamy EtaleditorijmrhsNo ratings yet
- 40vedant EtalDocument4 pages40vedant EtaleditorijmrhsNo ratings yet
- 37poflee EtalDocument3 pages37poflee EtaleditorijmrhsNo ratings yet
- 32bheemprasad EtalDocument3 pages32bheemprasad EtaleditorijmrhsNo ratings yet
- Pernicious Anemia in Young: A Case Report With Review of LiteratureDocument5 pagesPernicious Anemia in Young: A Case Report With Review of LiteratureeditorijmrhsNo ratings yet
- 36rashmipal EtalDocument6 pages36rashmipal EtaleditorijmrhsNo ratings yet
- 34tupe EtalDocument5 pages34tupe EtaleditorijmrhsNo ratings yet
- 33 Prabu RamDocument5 pages33 Prabu RameditorijmrhsNo ratings yet
- Universal Immunization ProgrammeDocument3 pagesUniversal Immunization ProgrammeAmy Lalringhluani ChhakchhuakNo ratings yet
- Practice Problems MCQDocument2 pagesPractice Problems MCQShilajit BaruaNo ratings yet
- VRC-VV Training BrochureDocument2 pagesVRC-VV Training BrochureKathiravan GopalanNo ratings yet
- Controle Global É TestadoDocument11 pagesControle Global É TestadoDavidson Leandro Silva dos SantosNo ratings yet
- Precipath HBA1C.12173514001.V12.en PDFDocument2 pagesPrecipath HBA1C.12173514001.V12.en PDFARIF AHAMMED PNo ratings yet
- 30 02 09 GrappasonniDocument11 pages30 02 09 GrappasonnielNo ratings yet
- Current MI Rabies MapDocument1 pageCurrent MI Rabies MapWDIV/ClickOnDetroitNo ratings yet
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocument2 pagesDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNo ratings yet
- Dermatologic Manifestations of Bacillary AngiomatosisDocument7 pagesDermatologic Manifestations of Bacillary AngiomatosisdrkayceeNo ratings yet
- CleanlinessDocument5 pagesCleanlinessAlark JogNo ratings yet
- Transes-Funda Rle PrelimsDocument12 pagesTranses-Funda Rle Prelimsmikhyla.cardenoNo ratings yet
- Treating UTIs and PneumoniaDocument1 pageTreating UTIs and PneumoniaNatalia SpencerNo ratings yet
- Wordlist medical termsDocument2 pagesWordlist medical termsEstherEscuderoNo ratings yet
- Pott Disease (TB Spondylitis) (Emed)Document7 pagesPott Disease (TB Spondylitis) (Emed)Ali Al.JuffairiNo ratings yet
- WHO Guidelines For Hand Hygiene in Health CareDocument216 pagesWHO Guidelines For Hand Hygiene in Health CarescretchyNo ratings yet
- Parte ADocument16 pagesParte AHelena VelezNo ratings yet
- Bacterial ConjunctivitisDocument32 pagesBacterial ConjunctivitisYouhengNo ratings yet
- Maternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoDocument8 pagesMaternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoLola del carmen RojasNo ratings yet
- Anti Mycobacterial DrugsDocument16 pagesAnti Mycobacterial DrugsIqra NaeemNo ratings yet
- Hypochlorous Acid (HOCl)Document5 pagesHypochlorous Acid (HOCl)andualemNo ratings yet
- Bio-Energetic Frequency ChartsDocument37 pagesBio-Energetic Frequency ChartsHayden JamesNo ratings yet
- Problem - Solving - Collected 2Document64 pagesProblem - Solving - Collected 2mulyadiNo ratings yet
- Privateroom JournalDocument5 pagesPrivateroom JournalNathaniel PulidoNo ratings yet