You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NCRA AJCC Cancer Staging Manual 8th Edition UpdateDocument61 pagesNCRA AJCC Cancer Staging Manual 8th Edition UpdateNancyLiao50% (2)
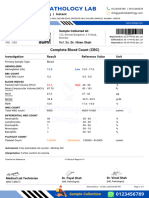
- CBC Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageCBC Test Report Format Example Sample Template Drlogy Lab ReportThota charanNo ratings yet
- Referat (PPT) - Hiperleukositosis & LeukostasisDocument16 pagesReferat (PPT) - Hiperleukositosis & LeukostasisShapira alNo ratings yet
- Topnotch Medical Juris For MoonlightersDocument78 pagesTopnotch Medical Juris For Moonlightersmefav7778520No ratings yet
- CMS CastleDocument5 pagesCMS CastleKian GonzagaNo ratings yet
- 002 Exsultet Choir PartsDocument2 pages002 Exsultet Choir PartsKian GonzagaNo ratings yet
- 000 Holy Saturday Extract From Priest Altar BookDocument45 pages000 Holy Saturday Extract From Priest Altar BookKian GonzagaNo ratings yet
- Basic Airway ManagmentDocument28 pagesBasic Airway ManagmentKian GonzagaNo ratings yet
- Firmly I Believe - SEMS - SATBDocument1 pageFirmly I Believe - SEMS - SATBKian GonzagaNo ratings yet
- Easter Sun 6A - Ps 65 (66) - Part 1Document1 pageEaster Sun 6A - Ps 65 (66) - Part 1Kian GonzagaNo ratings yet
- Revised Bishop Installation MassDocument43 pagesRevised Bishop Installation MassKian GonzagaNo ratings yet
- User Manual: Register Pay LearnDocument21 pagesUser Manual: Register Pay LearnKian GonzagaNo ratings yet
- Psalm and POFDocument1 pagePsalm and POFKian GonzagaNo ratings yet
- LS Intuity The Server Getting-StartedDocument38 pagesLS Intuity The Server Getting-StartedKian GonzagaNo ratings yet
- Highlights+Bar+Menu+ +With+Price+March+2021Document2 pagesHighlights+Bar+Menu+ +With+Price+March+2021Kian GonzagaNo ratings yet
- Check Out Our Digital Menus: Just Scan or Click On Below QR CodesDocument1 pageCheck Out Our Digital Menus: Just Scan or Click On Below QR CodesKian GonzagaNo ratings yet
- Learningspace Troubleshooting Guide: - Start HereDocument1 pageLearningspace Troubleshooting Guide: - Start HereKian GonzagaNo ratings yet
- Course: Patient Safety Solutions Topic:: Some DefinitionsDocument5 pagesCourse: Patient Safety Solutions Topic:: Some DefinitionsKian GonzagaNo ratings yet
- Show PRDocument1 pageShow PRKian GonzagaNo ratings yet
- Specs Features: FrameDocument1 pageSpecs Features: FrameKian GonzagaNo ratings yet
- ChargeTech PLUG Manual - 42K & 54KDocument6 pagesChargeTech PLUG Manual - 42K & 54KKian GonzagaNo ratings yet
- Light Vehicle enDocument8 pagesLight Vehicle enKian GonzagaNo ratings yet
- Belkin Manual PDFDocument43 pagesBelkin Manual PDFKian GonzagaNo ratings yet
- Bike Shop - MAP - 2020Document1 pageBike Shop - MAP - 2020Kian GonzagaNo ratings yet
- CAE Biography Rekha Ranganathan ENDocument1 pageCAE Biography Rekha Ranganathan ENKian GonzagaNo ratings yet
- ﻲﺒﻇﻮﺑأ ﺔﻃﺮﺷ تﺎﻣﺪﺧ ﻖﻴﺒﻄﺗ لﻼﺧ ﻦﻣ ﻒﻠﻤﻟا ﺔﻛرﺎﺸﻣ ﻢﺗ Generated through Abu Dhabi Police mobile applicationDocument1 pageﻲﺒﻇﻮﺑأ ﺔﻃﺮﺷ تﺎﻣﺪﺧ ﻖﻴﺒﻄﺗ لﻼﺧ ﻦﻣ ﻒﻠﻤﻟا ﺔﻛرﺎﺸﻣ ﻢﺗ Generated through Abu Dhabi Police mobile applicationKian GonzagaNo ratings yet
- PPI-851712f Patient Advance Receipt PDFDocument1 pagePPI-851712f Patient Advance Receipt PDFKian GonzagaNo ratings yet
- Clinical Paper: The Management of Impacted Third Molar TeethDocument4 pagesClinical Paper: The Management of Impacted Third Molar TeethAkmal HafizhNo ratings yet
- SchematicDocument18 pagesSchematicfabiofiss4795No ratings yet
- Comments: LPL - PSC Narela Shop No: B-17, U-59, RK Plaza, Lampur ROAD Mob: 9582019820 DelhiDocument1 pageComments: LPL - PSC Narela Shop No: B-17, U-59, RK Plaza, Lampur ROAD Mob: 9582019820 DelhiBhaskar RanjanNo ratings yet
- PSMA in Seminal Vesicle AmyloidDocument2 pagesPSMA in Seminal Vesicle AmyloidGaurav MalhotraNo ratings yet
- Blood Bank Data Collection FormDocument3 pagesBlood Bank Data Collection Formpbta punjab100% (1)
- Blood GroupDocument44 pagesBlood Groupmujtaba100% (2)
- Venkatraman K PDFDocument3 pagesVenkatraman K PDFRana Zara AthayaNo ratings yet
- Vedhanshi Medical Laboratory - CDCTS16 Hanamkonda - 30Document1 pageVedhanshi Medical Laboratory - CDCTS16 Hanamkonda - 30vijaykumarNo ratings yet
- 49 Alcare Website: Permanent No. Referred by Pat. Address: Ms. Sneha Saikia: 486069 Lab No. Age / SexDocument1 page49 Alcare Website: Permanent No. Referred by Pat. Address: Ms. Sneha Saikia: 486069 Lab No. Age / SexTina SaikiaNo ratings yet
- Certificate IV in PathologyDocument6 pagesCertificate IV in PathologyUpul EdirisingheNo ratings yet
- His To PathologyDocument52 pagesHis To PathologyRathinaKumarNo ratings yet
- Echocardiography & Color Doppler Report Measurements Absolute Value Normals Absolute / MDocument3 pagesEchocardiography & Color Doppler Report Measurements Absolute Value Normals Absolute / MAmol PandeyNo ratings yet
- Fibroadenoma Versus Phyllodes TumorDocument12 pagesFibroadenoma Versus Phyllodes TumorNatalindah Jokiem Woecandra T. D.No ratings yet
- Prelim HPCTDocument37 pagesPrelim HPCTMariaangela AliscuanoNo ratings yet
- Mak Roo 2018Document7 pagesMak Roo 2018my accountNo ratings yet
- ESIMasterJournalList 082018 1Document783 pagesESIMasterJournalList 082018 1bapaknyanadlirNo ratings yet
- Beginings of MTDocument65 pagesBeginings of MTMel JamitoNo ratings yet
- Blood Typing PresentationDocument39 pagesBlood Typing PresentationNezzeh Clair D. BermejoNo ratings yet
- Lab Scope of ServicesDocument10 pagesLab Scope of Servicessabir osmanNo ratings yet
- The Role of Ioc in Sarcoma SurgeryDocument31 pagesThe Role of Ioc in Sarcoma SurgeryLILA RUSTIKANo ratings yet
- PATH310Document6 pagesPATH310Emmanuel EsedafeNo ratings yet
- RedbookDocument286 pagesRedbookĐỗ Lê Đức ThuậnNo ratings yet
- Mrs. V.dhana LakshmiDocument1 pageMrs. V.dhana LakshmiAnonymous lSZ9JVNo ratings yet
- Shalakya Tantra SyllabusDocument65 pagesShalakya Tantra SyllabusIshwari GaikwadNo ratings yet
- Medical Technology: (1) History of The Medical Laboratory ScienceDocument63 pagesMedical Technology: (1) History of The Medical Laboratory ScienceJAKE DANGPASONNo ratings yet
- Bladder 4.1.0.0.rel CapcpDocument19 pagesBladder 4.1.0.0.rel CapcpkarimahihdaNo ratings yet