You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- BioceramicsDocument27 pagesBioceramicsAlexander DavidNo ratings yet
- Management of Acute Severe Traumatic Brain InjuryDocument24 pagesManagement of Acute Severe Traumatic Brain InjuryLidya ChristyNo ratings yet
- The Correlation Between Parenting Style and Child StuntingDocument15 pagesThe Correlation Between Parenting Style and Child StuntingMonica RaharjoNo ratings yet
- Neurology of COVID 19Document330 pagesNeurology of COVID 19Daniel Mamani CruzNo ratings yet
- Blood Can Be Very BadDocument37 pagesBlood Can Be Very BadPhil SingerNo ratings yet
- Oxford Handbook of Medical Dermatology (Oxford Medical Handbooks) PDF DownloadDocument2 pagesOxford Handbook of Medical Dermatology (Oxford Medical Handbooks) PDF Downloadwang lembak0% (5)
- Clinical Sciences Study PlanDocument30 pagesClinical Sciences Study PlanRomulo Vincent PerezNo ratings yet
- Challenges In Obstetric Anesthesia: 10 Key Issues for CRNAsDocument38 pagesChallenges In Obstetric Anesthesia: 10 Key Issues for CRNAsPaulHerreraNo ratings yet
- Staff Nurse Job ApplicationDocument10 pagesStaff Nurse Job ApplicationArvenaa SubramaniamNo ratings yet
- Full Report - ELISA LatestDocument8 pagesFull Report - ELISA LatestNik AmirNo ratings yet
- Diagnosis Dan Pengobatan Reaksi Kusta Di Layanan Terpadu - Perspektif Pasien Di NepalDocument1 pageDiagnosis Dan Pengobatan Reaksi Kusta Di Layanan Terpadu - Perspektif Pasien Di NepalBernad NauliNo ratings yet
- Traumatic Brain Injury - Epidemiology, Classification, and PathophysiologyDocument12 pagesTraumatic Brain Injury - Epidemiology, Classification, and PathophysiologyLidya ChristyNo ratings yet
- HE PJKDocument26 pagesHE PJKLidya ChristyNo ratings yet
- Dengue Guideline DengueDocument33 pagesDengue Guideline DenguedrkkdbNo ratings yet
- ACME Quote-Word 2003Document4 pagesACME Quote-Word 2003Mutmainnah AGNo ratings yet
- 08-04-15 Data MH Jan 2012 - Jan 2015Document15 pages08-04-15 Data MH Jan 2012 - Jan 2015Lidya ChristyNo ratings yet
- Nej Mo A 1213096Document9 pagesNej Mo A 1213096Lidya ChristyNo ratings yet
- Drug and Multidrug Resistance Among Mycobacterium Leprae Isolates From Brazilian Relapsed Leprosy PatientsDocument6 pagesDrug and Multidrug Resistance Among Mycobacterium Leprae Isolates From Brazilian Relapsed Leprosy PatientsLidya ChristyNo ratings yet
- Temporal Adverse Effects in Leprosy Saudi Patients Receiving Multi Drug Therapy 2161 1459-3-141Document4 pagesTemporal Adverse Effects in Leprosy Saudi Patients Receiving Multi Drug Therapy 2161 1459-3-141Lidya ChristyNo ratings yet
- Morning Report 21-5Document14 pagesMorning Report 21-5Lidya ChristyNo ratings yet
- 1471 2334 13 456Document8 pages1471 2334 13 456Lidya ChristyNo ratings yet
- Journal - Pone.0105785 AMI&ACIDocument9 pagesJournal - Pone.0105785 AMI&ACILidya ChristyNo ratings yet
- Is There A Role For Rifampicin, Ofloxacin and Minocycline (ROM) Therapy in The Treatment of Leprosy? Systematic Review and Meta-AnalysisDocument11 pagesIs There A Role For Rifampicin, Ofloxacin and Minocycline (ROM) Therapy in The Treatment of Leprosy? Systematic Review and Meta-AnalysisLidya ChristyNo ratings yet
- Is There A Role For Rifampicin, Ofloxacin and Minocycline (ROM) Therapy in The Treatment of Leprosy? Systematic Review and Meta-AnalysisDocument11 pagesIs There A Role For Rifampicin, Ofloxacin and Minocycline (ROM) Therapy in The Treatment of Leprosy? Systematic Review and Meta-AnalysisLidya ChristyNo ratings yet
- Morning Report 21-5Document14 pagesMorning Report 21-5Lidya ChristyNo ratings yet
- Spontaneous Intracerebral Hemorrhage - Treatment and PrognosisDocument22 pagesSpontaneous Intracerebral Hemorrhage - Treatment and PrognosisLidya ChristyNo ratings yet
- Spontaneous Intracerebral Hemorrhage - Treatment and PrognosisDocument22 pagesSpontaneous Intracerebral Hemorrhage - Treatment and PrognosisLidya ChristyNo ratings yet
- Journal - Pone.0105785 AMI&ACIDocument9 pagesJournal - Pone.0105785 AMI&ACILidya ChristyNo ratings yet
- Overview of The Management of Epilepsy in AdultsDocument29 pagesOverview of The Management of Epilepsy in AdultsLidya ChristyNo ratings yet
- What Is EdemaDocument3 pagesWhat Is EdemaLidya ChristyNo ratings yet
- Risk Factors For Severe Acute Lower Respiratory Tract Infection in Under-Five ChildrenDocument10 pagesRisk Factors For Severe Acute Lower Respiratory Tract Infection in Under-Five ChildrenLidya ChristyNo ratings yet
- Design PPT (K)Document20 pagesDesign PPT (K)Lidya ChristyNo ratings yet
- Case Report Negative Rusell Body GastritisDocument3 pagesCase Report Negative Rusell Body GastritisLidya ChristyNo ratings yet
- Risk Factors For Severe Acute Lower Respiratory Tract Infection in Under-Five ChildrenDocument10 pagesRisk Factors For Severe Acute Lower Respiratory Tract Infection in Under-Five ChildrenLidya ChristyNo ratings yet
- How Breast Milk Protects NewbornsDocument4 pagesHow Breast Milk Protects NewbornsDennis HerreraNo ratings yet
- Cover Kasus 4-ForENSIKDocument1 pageCover Kasus 4-ForENSIKTri AriyaniNo ratings yet
- What Is EdemaDocument3 pagesWhat Is EdemaLidya ChristyNo ratings yet
- Patofisiologi Ulkus VarikosumDocument5 pagesPatofisiologi Ulkus VarikosumLidya ChristyNo ratings yet
- Abo IncompatabilityDocument3 pagesAbo Incompatabilityx483xDNo ratings yet
- CRT BacteriaDocument15 pagesCRT BacteriatsntiNo ratings yet
- PreviewpdfDocument481 pagesPreviewpdfAdams BrunoNo ratings yet
- Postural, DrainageDocument7 pagesPostural, DrainageJames ThompsonNo ratings yet
- Child Abuse 3Document9 pagesChild Abuse 3Nilsa RoblesNo ratings yet
- Basketball InjuriesDocument2 pagesBasketball Injuriesapi-335139173No ratings yet
- A Survey of Stent Designs PDFDocument11 pagesA Survey of Stent Designs PDFGabriel Lopez BarajasNo ratings yet
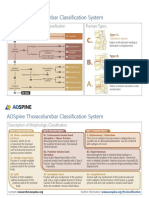
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 pagesAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Beat Tonsil BookDocument19 pagesBeat Tonsil BookXheni MeleNo ratings yet
- 136 137 Plastic Surgery The FutureDocument2 pages136 137 Plastic Surgery The FutureShirley KoehNo ratings yet
- Basics Of Ayurvedic PharmacologyDocument3 pagesBasics Of Ayurvedic PharmacologySN Wijesinhe100% (1)
- Resme Rahul GuptaDocument5 pagesResme Rahul Guptarahul guptaNo ratings yet
- Principles of Posterior Fossa Surgery 2012Document269 pagesPrinciples of Posterior Fossa Surgery 2012Alexandru GolesteanuNo ratings yet
- Current Immunization Schedule of Routine Epi in PakistanDocument2 pagesCurrent Immunization Schedule of Routine Epi in PakistanDilawar JanNo ratings yet
- List of Surgeons ThereferencelistDocument4 pagesList of Surgeons Thereferencelistapi-367609425No ratings yet
- IPMN of The PancreasDocument12 pagesIPMN of The PancreasLúcia FarrachoNo ratings yet
- Definitions of Orthodontic TermsDocument10 pagesDefinitions of Orthodontic TermsFirda HandayaniNo ratings yet
- Upgrading a 63-Year-Old Philippine Public HospitalDocument77 pagesUpgrading a 63-Year-Old Philippine Public HospitalMark Ryan NagalesNo ratings yet
- Children and Neonates Anesthesia in Magnetic Resonance Environment in Italy - BMC Anest22Document9 pagesChildren and Neonates Anesthesia in Magnetic Resonance Environment in Italy - BMC Anest22Gunther MirandaNo ratings yet
- Current Concepts: Scapular Dyskinesis: W Ben Kibler, Aaron SciasciaDocument7 pagesCurrent Concepts: Scapular Dyskinesis: W Ben Kibler, Aaron SciasciatomxtchNo ratings yet
- 11 01 06 Bambach BrochureDocument6 pages11 01 06 Bambach BrochureFred StoreyNo ratings yet