You might also like
- ImproNES Dadfsdfsdfsdfsd DFSDFSD Fasdfa SDFDocument1 pageImproNES Dadfsdfsdfsdfsd DFSDFSD Fasdfa SDFRye AnchNo ratings yet
- Aditional Client PresDocument2 pagesAditional Client PresRye AnchNo ratings yet
- Some Useful QuotesDocument1 pageSome Useful QuotesRye AnchNo ratings yet
- Alternative Treatment For Parkinson's DiseaseDocument3 pagesAlternative Treatment For Parkinson's DiseaseRye AnchNo ratings yet
- Alcohol Related DisordersDocument14 pagesAlcohol Related DisordersRye AnchNo ratings yet
- Attention Deficit Hyperactivity DisorderDocument9 pagesAttention Deficit Hyperactivity DisorderRye AnchNo ratings yet
- Abstract Pathophysiology of Gun Shot Wound On The BrainDocument1 pageAbstract Pathophysiology of Gun Shot Wound On The BrainRye AnchNo ratings yet
- Drug ListDocument1 pageDrug ListRye AnchNo ratings yet
- VS Easy VS PaperDocument1 pageVS Easy VS PaperRye AnchNo ratings yet
- Calcium CarbonateDocument1 pageCalcium CarbonateRye AnchNo ratings yet
- Drug StudyDocument8 pagesDrug StudyRye AnchNo ratings yet
- Omeprazole Drug StudyDocument2 pagesOmeprazole Drug StudyRye Anch75% (8)
- Client PressentationDocument2 pagesClient PressentationRye AnchNo ratings yet
- Pathophysiology PTBDocument4 pagesPathophysiology PTBRye AnchNo ratings yet
- DrugsDocument7 pagesDrugsRye AnchNo ratings yet
- VancomycinDocument2 pagesVancomycinRye AnchNo ratings yet
- Ok Psychomotor SkillsDocument1 pageOk Psychomotor SkillsRye AnchNo ratings yet
- Taking Action To Close The Nursing-Finance Gap: Learning From SuccessDocument3 pagesTaking Action To Close The Nursing-Finance Gap: Learning From SuccessRye Anch100% (1)
- Erce FloraDocument2 pagesErce FloraRye Anch0% (1)
- Atorvastatin Drug StudyDocument2 pagesAtorvastatin Drug StudyRye Anch88% (17)
- Bailen - FNCPDocument2 pagesBailen - FNCPRye AnchNo ratings yet
- Omeprazole Drug StudyDocument2 pagesOmeprazole Drug StudyRye Anch75% (8)
- Tramadol Hydrochloride (Ultran, Ultracet)Document1 pageTramadol Hydrochloride (Ultran, Ultracet)Rye AnchNo ratings yet
- Physical Assessment Compilation FinalDocument13 pagesPhysical Assessment Compilation FinalRye AnchNo ratings yet
- DfasdfasdfasdfasdfaDocument2 pagesDfasdfasdfasdfasdfaRye AnchNo ratings yet
- Conditions That Can Beconsidered ABCDocument4 pagesConditions That Can Beconsidered ABCRye AnchNo ratings yet
- VideoasdfasdfasdfasdfaDocument1 pageVideoasdfasdfasdfasdfaRye AnchNo ratings yet
- Tramadol Hydrochloride (Ultran, Ultracet)Document1 pageTramadol Hydrochloride (Ultran, Ultracet)Rye AnchNo ratings yet
- HYDROXYZINE DIHCL (Iterax)Document1 pageHYDROXYZINE DIHCL (Iterax)Rye Anch100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chapter 8 - Transport in MammalsDocument119 pagesChapter 8 - Transport in Mammalsapi-3728508100% (1)
- Spinal Cord Injury and Compression PDFDocument6 pagesSpinal Cord Injury and Compression PDFRem AlfelorNo ratings yet
- Bender Pulpal Pain Diagnosis ReviewDocument5 pagesBender Pulpal Pain Diagnosis ReviewSilvia SolisNo ratings yet
- Human BodyDocument2 pagesHuman BodyvuppalasampathNo ratings yet
- Revisiting Molar DistalizationDocument4 pagesRevisiting Molar DistalizationPARIJAT CHAKRABORTYNo ratings yet
- HirudinomorphaDocument3 pagesHirudinomorphaDave RapaconNo ratings yet
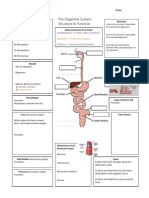
- The Digestive SystemDocument38 pagesThe Digestive SystemrabiaNo ratings yet
- Neuro Endo QuestionsDocument45 pagesNeuro Endo Questionsmayor_saadNo ratings yet
- MY CLASS NOTES - BIOLOGY Circulatory SystemDocument3 pagesMY CLASS NOTES - BIOLOGY Circulatory SystemJjongNo ratings yet
- Liver PathologyDocument9 pagesLiver PathologyAman BasidaNo ratings yet
- اسايمنت البيدوDocument2 pagesاسايمنت البيدوTasneem AbdNo ratings yet
- Cure Your Migraines The Natural WayDocument220 pagesCure Your Migraines The Natural WayAggie E KrolNo ratings yet
- The Digestive System Graphic OrganiserDocument1 pageThe Digestive System Graphic Organiserapi-350307578100% (1)
- Monday Neuroscience ProgramDocument183 pagesMonday Neuroscience ProgramAlfonso Fajardo0% (1)
- Occlusion in Complete DentureDocument57 pagesOcclusion in Complete DentureSahana Rangarajan100% (1)
- 20) Dr. Dr. Himawan Sanusi, Sp. PD, KEMD - Cushing+conn+addsosnianDocument27 pages20) Dr. Dr. Himawan Sanusi, Sp. PD, KEMD - Cushing+conn+addsosnianAsridewi DewiNo ratings yet
- Notes: Generally, What Are They?Document10 pagesNotes: Generally, What Are They?Yusril MarhaenNo ratings yet
- (1 Point) : Elevation of BBTDocument7 pages(1 Point) : Elevation of BBTgelean payodNo ratings yet
- Upper Airway Anatomy and FunctionDocument86 pagesUpper Airway Anatomy and FunctionekaefkaNo ratings yet
- Physiological and Psychological Changes During PregnancyDocument3 pagesPhysiological and Psychological Changes During Pregnancykimglaidyl bontuyanNo ratings yet
- CIRCULATION PHYSIOLOGY MCQs Test PDFDocument6 pagesCIRCULATION PHYSIOLOGY MCQs Test PDFMiles Hui67% (3)
- Cardiovascular System PPT FeDocument26 pagesCardiovascular System PPT FeAngel Grace GaliasNo ratings yet
- BioPsych Lecture Notes CH 7Document6 pagesBioPsych Lecture Notes CH 7Generic_Persona100% (1)
- Anatomy of The CVS: ThoraxDocument10 pagesAnatomy of The CVS: ThoraxNayerShammaaNo ratings yet
- Renal System 6 1Document30 pagesRenal System 6 1gaurav singhNo ratings yet
- Assignment Physiology Name:: Nowal ChoudharyDocument12 pagesAssignment Physiology Name:: Nowal ChoudharyhammdNo ratings yet
- Cementogenesis: DR Saqlain Bin Syed GilaniDocument12 pagesCementogenesis: DR Saqlain Bin Syed GilaniNatasha BalochNo ratings yet
- Brain PartsDocument11 pagesBrain PartsTuesday SacdalanNo ratings yet
- Word Roots and Combining Forms For AnatomyDocument7 pagesWord Roots and Combining Forms For AnatomyDavid HosamNo ratings yet
- Broderick Occlusal Plane Analyzer (1DIEGO)Document5 pagesBroderick Occlusal Plane Analyzer (1DIEGO)diegoNo ratings yet