You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Heart Failure Review QuestionsDocument33 pagesHeart Failure Review Questionszbestgurl100% (2)
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (2)
- AbbreviationDocument19 pagesAbbreviationJayson NatividadNo ratings yet
- The Cleveland Clinic Cardiology Board ReviewDocument114 pagesThe Cleveland Clinic Cardiology Board ReviewSohil Elfar100% (1)
- HAAD Q and ADocument100 pagesHAAD Q and Aleah100% (24)
- Medical SurgicalDocument10 pagesMedical Surgicalclobregas100% (1)
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Nursing Management of Patient With CCFDocument34 pagesNursing Management of Patient With CCFJayarani Ashok100% (1)
- List of AbreviationDocument44 pagesList of Abreviationdapsjen deadNo ratings yet
- Geria - CardioDocument4 pagesGeria - CardioLeah GordoncilloNo ratings yet
- IM HandbookaDocument378 pagesIM HandbookakkNo ratings yet
- HSNS362Document16 pagesHSNS362mandyNo ratings yet
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
- Annals: OF SurgeryDocument5 pagesAnnals: OF SurgeryqisthiaufaNo ratings yet
- Steroid WikiDocument16 pagesSteroid WikiqisthiaufaNo ratings yet
- Cover FER 4Document1 pageCover FER 4qisthiaufaNo ratings yet
- Ajpregu 00176 2014 FullDocument9 pagesAjpregu 00176 2014 FullqisthiaufaNo ratings yet
- Obstetrics 2Document10 pagesObstetrics 2qisthiaufaNo ratings yet
- Case Report: Eisenmenger Syndrome in PregnancyDocument2 pagesCase Report: Eisenmenger Syndrome in PregnancyqisthiaufaNo ratings yet
- Umbilical Cord Blood Gas AnalysisDocument2 pagesUmbilical Cord Blood Gas AnalysisqisthiaufaNo ratings yet
- Routine Testing of Umbilical Cord Blood After Normal DeliveryDocument2 pagesRoutine Testing of Umbilical Cord Blood After Normal DeliveryqisthiaufaNo ratings yet
- Cardiac (Heart) TransplantationDocument9 pagesCardiac (Heart) TransplantationXristos BeretisNo ratings yet
- CD's Reddit Step 1 PlanDocument44 pagesCD's Reddit Step 1 PlanMohammad NabeelNo ratings yet
- TCHP-Docetaxel Carboplatin Trastuzumab Pertuzumab Neoadjuvant Adjuvant Protocol V2.2Document21 pagesTCHP-Docetaxel Carboplatin Trastuzumab Pertuzumab Neoadjuvant Adjuvant Protocol V2.2smokkerNo ratings yet
- CPG - Acute Pulmonary OedemaDocument4 pagesCPG - Acute Pulmonary OedemaAmalinaNo ratings yet
- Pulm Circ - 2013 - Forfia - Pulmonary Heart Disease The Heart Lung Interaction and Its Impact On Patient PhenotypesDocument15 pagesPulm Circ - 2013 - Forfia - Pulmonary Heart Disease The Heart Lung Interaction and Its Impact On Patient PhenotypesFanugrahNo ratings yet
- 1 s2.0 S0828282X22001271 MainDocument11 pages1 s2.0 S0828282X22001271 MainLilianne Mbengani LaranjeiraNo ratings yet
- Clinical Pharmacology of Dobutamine and Dopamine in Preterm NeonatesDocument9 pagesClinical Pharmacology of Dobutamine and Dopamine in Preterm Neonatesmateri posNo ratings yet
- Suspected Heart Failure: Section 5 Section 7 Section 8Document10 pagesSuspected Heart Failure: Section 5 Section 7 Section 8Javier TapiaNo ratings yet
- Dilated Cardiomyopathy Notes AtfDocument15 pagesDilated Cardiomyopathy Notes AtfSingha ChangsiriwatanaNo ratings yet
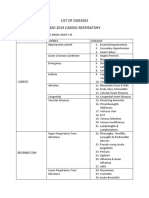
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- 1 s2.0 S2772632022000496 MainDocument8 pages1 s2.0 S2772632022000496 MainaminNo ratings yet
- CME - Breathlessness RadDocument51 pagesCME - Breathlessness Radjun sianNo ratings yet
- Causes and Evaluation of Hyperkalemia in AdultsDocument25 pagesCauses and Evaluation of Hyperkalemia in AdultsAnonymous iAoPnb2sNo ratings yet
- CHF CSDocument4 pagesCHF CSLaren CyrNo ratings yet
- ANN Online CourseDocument7 pagesANN Online CourseJovan Varona NealaNo ratings yet
- Teaching Rounds A Visual Aid To Teaching Internal Medicine Pearls On The Wards 1St Edition Navin Kumar Full ChapterDocument67 pagesTeaching Rounds A Visual Aid To Teaching Internal Medicine Pearls On The Wards 1St Edition Navin Kumar Full Chapterbertha.commings489100% (7)
- ACE Inhibitors & Angiotensin II Antagonists: October 1997Document4 pagesACE Inhibitors & Angiotensin II Antagonists: October 1997indee533No ratings yet