You might also like
- Korumasız LMCA Girişimleri - Murat ÇaylıDocument45 pagesKorumasız LMCA Girişimleri - Murat ÇaylıAlpBurakÇatakoğluNo ratings yet
- Adaptif Radyoterapi (ART)Document81 pagesAdaptif Radyoterapi (ART)Mehtap CoskunNo ratings yet
- İleri Kardiyak Yaşam Desteği YenilikleriDocument45 pagesİleri Kardiyak Yaşam Desteği YeniliklerigoktugNo ratings yet
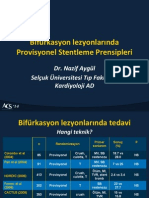
- Provizyonel Stentleme - Nazif AygülDocument10 pagesProvizyonel Stentleme - Nazif AygülAlpBurakÇatakoğluNo ratings yet
- Turkce Ders NotlariDocument92 pagesTurkce Ders Notlariabidik123No ratings yet
- Icru 50-62Document34 pagesIcru 50-62Ahmet Kürşat ÖzkanNo ratings yet
- D3-4-Düzensiz Alanlar, Bloklar, Bitişik Alanlar - Tedavi PlanlamaDocument110 pagesD3-4-Düzensiz Alanlar, Bloklar, Bitişik Alanlar - Tedavi PlanlamaAslı AioiaiNo ratings yet
- Calcaneal FracturesDocument25 pagesCalcaneal FracturesNizami TİMURNo ratings yet
- STENTsunumDocument26 pagesSTENTsunumGhadir NoriNo ratings yet
- Nodal Oligorekürrent Prostat Kanserinde Elektif Nodal Radyoterapi Ve Stereotaktik Beden Radyoterapisinin KarşılaştırılmasıDocument23 pagesNodal Oligorekürrent Prostat Kanserinde Elektif Nodal Radyoterapi Ve Stereotaktik Beden Radyoterapisinin KarşılaştırılmasıDoğa AkaoğluNo ratings yet
- CBS Cronicas TRDocument45 pagesCBS Cronicas TRFortinNo ratings yet
- Ders 5 - Göz Ve Prostat UygulamalariDocument40 pagesDers 5 - Göz Ve Prostat Uygulamalariyns.srlNo ratings yet
- ImplantolojiDocument93 pagesImplantolojiFırat KöseNo ratings yet
- Ders 3 - Interstisyel BT de Dozimetri Sistemleri - 15042013Document41 pagesDers 3 - Interstisyel BT de Dozimetri Sistemleri - 15042013yns.srlNo ratings yet
- Vista 120 S Pi 9104171Document14 pagesVista 120 S Pi 9104171hüseyin vururNo ratings yet
- Ders 1-2-Radyoterapinin Tanımı, AmacıDocument77 pagesDers 1-2-Radyoterapinin Tanımı, AmacıÖmerBahadırMergenNo ratings yet
- Omurgada Semptomatik Yükseklik Kaybı Nedeniyle Kifoplasti Uyguladığımız Hastalarda SonuçlarımızDocument6 pagesOmurgada Semptomatik Yükseklik Kaybı Nedeniyle Kifoplasti Uyguladığımız Hastalarda SonuçlarımızBilal ErtugrulNo ratings yet
- AkciÄ Er Kanseri Rad Onk 1Document17 pagesAkciÄ Er Kanseri Rad Onk 1Nursena ÇiflikNo ratings yet
- Yetişkinlerde Mandibular Kondil Kiriklarina Cerrahi Tedavi YaklaşimiDocument81 pagesYetişkinlerde Mandibular Kondil Kiriklarina Cerrahi Tedavi YaklaşimimustafasacarNo ratings yet
- Olgu GSCKDocument40 pagesOlgu GSCKChristine HudginsNo ratings yet
- 2023-2024 İngi̇li̇zce A Grubu Noroloji̇ ÇikmişlarDocument4 pages2023-2024 İngi̇li̇zce A Grubu Noroloji̇ Çikmişlarkiritokirito1212No ratings yet
- Skopi̇k İşlemler-Turkrad2019-Kaan AtacDocument33 pagesSkopi̇k İşlemler-Turkrad2019-Kaan AtacKaan CHDRNo ratings yet
- 06 - Akut Aortik SendromlarDocument65 pages06 - Akut Aortik SendromlarAlp HatNo ratings yet
- Karotis IşlemlerDocument16 pagesKarotis Işlemlersinan inciNo ratings yet
- Akut Koroner Sendrom-1Document112 pagesAkut Koroner Sendrom-1Yasin Yıldız100% (1)
- Çocuklarda Omurga Hastalıkları-30.03.2022 - M.özerDocument56 pagesÇocuklarda Omurga Hastalıkları-30.03.2022 - M.özermehmet ÖzerNo ratings yet
- Meme Karsi̇nomuDocument74 pagesMeme Karsi̇nomuMona LisaNo ratings yet
- Damar YoluDocument51 pagesDamar Yoluonukvedat7219No ratings yet
- Pulmoner Emboli,: DR - Gökçe Kaan Ataç Ufuk Üniversitesi Radyoloji ADDocument22 pagesPulmoner Emboli,: DR - Gökçe Kaan Ataç Ufuk Üniversitesi Radyoloji ADKaan CHDRNo ratings yet
- OnkolojikgörüntülemegirişDocument36 pagesOnkolojikgörüntülemegirişKaan CHDRNo ratings yet
- Mustafa Tez SunumDocument57 pagesMustafa Tez SunumkaratasmustafaaliNo ratings yet
- 4 Kardi̇yoloji̇ SorulariDocument97 pages4 Kardi̇yoloji̇ SorulariSalih ÇayırNo ratings yet
- DKT206 - Norodilbilim - 5. Hafta PDFDocument10 pagesDKT206 - Norodilbilim - 5. Hafta PDFOzgun KosanerNo ratings yet
- Bara Di̇feransi̇yel Koruma Tekni̇ği̇Document7 pagesBara Di̇feransi̇yel Koruma Tekni̇ği̇karaislimNo ratings yet
- Ko Mrfizik DönüştürüldüDocument133 pagesKo Mrfizik DönüştürüldünikaNo ratings yet
- Epstakss Salh Bakir KBB NotlariDocument6 pagesEpstakss Salh Bakir KBB Notlaridrmstfkrdnz6No ratings yet
- Tahribatsız Muayene PDFDocument32 pagesTahribatsız Muayene PDFFeratNo ratings yet
- Ventri̇küler Septal DefektDocument47 pagesVentri̇küler Septal Defektyiğit çangaNo ratings yet
- 17) Solunum Sistemi MonitörizasyonuDocument48 pages17) Solunum Sistemi Monitörizasyonuhalitgurel99No ratings yet
- Kardiyolojiozel14 2 3Document6 pagesKardiyolojiozel14 2 3Mathew McCarthyNo ratings yet
- Ecmo PDFDocument35 pagesEcmo PDFPiotr SerbanNo ratings yet
- KİBAS235Document50 pagesKİBAS235eceNo ratings yet
- cerrahide kan yönetimi 2021 - TÜRKÇEDocument49 pagescerrahide kan yönetimi 2021 - TÜRKÇESeda KaraçamNo ratings yet
- 12.05.2023 Ulcus CrurisDocument57 pages12.05.2023 Ulcus CrurisSemih AydemirNo ratings yet
- Mitral Kapak Tamirleri - Mustafa GüdenDocument22 pagesMitral Kapak Tamirleri - Mustafa GüdenAlpBurakÇatakoğluNo ratings yet
- PİCCO2 Türkçe KatologDocument8 pagesPİCCO2 Türkçe Katologferhat soykanNo ratings yet
- XB Idl SYe TD NIDocument76 pagesXB Idl SYe TD NIRamazan DoğanNo ratings yet
- Aile 84f3dDocument55 pagesAile 84f3dSedaNo ratings yet
- Aort Anevri̇zmasi Ve Di̇seksi̇yonu SunumuDocument54 pagesAort Anevri̇zmasi Ve Di̇seksi̇yonu SunumuÖmer Asım KahyaoğluNo ratings yet
- OtotoksisiteDocument43 pagesOtotoksisiteAtılım AtılganNo ratings yet
- 2 - Bladder TumorDocument34 pages2 - Bladder Tumorwd8gqspc5hNo ratings yet
- 4 Fetal İyi̇li̇k Hali̇ni̇n Değerlendi̇ri̇lmesi̇Document54 pages4 Fetal İyi̇li̇k Hali̇ni̇n Değerlendi̇ri̇lmesi̇hamad acheneNo ratings yet
- Febril Nötropenik Hastada Tanı Ve Risk Değerlendirmesi Mükremin UYSALDocument28 pagesFebril Nötropenik Hastada Tanı Ve Risk Değerlendirmesi Mükremin UYSALahmedNo ratings yet
- Radiobiology 4Document29 pagesRadiobiology 4Kaan CHDRNo ratings yet
- Radyoterapi CihazlarıDocument86 pagesRadyoterapi Cihazlarıhobiidunyasi372No ratings yet
- 04 - Geniş QRS TaşikardilerDocument62 pages04 - Geniş QRS TaşikardilerAlp HatNo ratings yet
- RadyolojiDocument69 pagesRadyolojiKemal Soysal100% (1)
- İçerikDocument60 pagesİçerikfeyzaNo ratings yet
- 703646Document59 pages703646Çağatay BozkurtNo ratings yet
- TAVI'de EKO - Yelda TayyareciDocument33 pagesTAVI'de EKO - Yelda TayyareciAlpBurakÇatakoğluNo ratings yet
- TAVI - Aydın YıldırımDocument74 pagesTAVI - Aydın YıldırımAlpBurakÇatakoğluNo ratings yet
- Mitral Kapak Tamirleri - Mustafa GüdenDocument22 pagesMitral Kapak Tamirleri - Mustafa GüdenAlpBurakÇatakoğluNo ratings yet
- STEMI'de Trombüsle Mücadele - Ertuğrul OkuyanDocument113 pagesSTEMI'de Trombüsle Mücadele - Ertuğrul OkuyanAlpBurakÇatakoğluNo ratings yet
- Kalp Konseyi Olgu SunumuDocument34 pagesKalp Konseyi Olgu SunumuAlpBurakÇatakoğluNo ratings yet
- STEMI'de Sorumlu Lezyon - Ali Metin EsenDocument40 pagesSTEMI'de Sorumlu Lezyon - Ali Metin EsenAlpBurakÇatakoğluNo ratings yet
- Iki Stent Teknikleri - Mehmet ErenDocument6 pagesIki Stent Teknikleri - Mehmet ErenAlpBurakÇatakoğluNo ratings yet
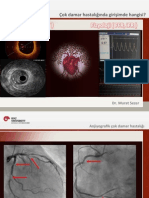
- Çok Damar Hastalığı Görüntüleme - Murat SezerDocument35 pagesÇok Damar Hastalığı Görüntüleme - Murat SezerAlpBurakÇatakoğluNo ratings yet
- BVS Üstün Müdür - Alp Burak CatakogluDocument52 pagesBVS Üstün Müdür - Alp Burak CatakogluAlpBurakÇatakoğluNo ratings yet
- Canlı Olgu SunumuDocument32 pagesCanlı Olgu SunumuAlpBurakÇatakoğluNo ratings yet
- Bifurkasyonda OCT - Gültekin HobikoğluDocument12 pagesBifurkasyonda OCT - Gültekin HobikoğluAlpBurakÇatakoğluNo ratings yet
- AF'de YOAK - Okan ErdoğanDocument14 pagesAF'de YOAK - Okan ErdoğanAlpBurakÇatakoğluNo ratings yet