You might also like
- NAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)From EverandNAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)Rating: 4.5 out of 5 stars4.5/5 (3)
- 1 Prof Chauvins Instructions For Bingham CH 4Document35 pages1 Prof Chauvins Instructions For Bingham CH 4Danielle Baldwin100% (2)
- The Beta-Blocker Story: Getting It RightFrom EverandThe Beta-Blocker Story: Getting It RightRating: 5 out of 5 stars5/5 (1)
- Roland Fantom s88Document51 pagesRoland Fantom s88harryoliff2672100% (1)
- Outpatient MedicineDocument190 pagesOutpatient MedicineLikoh TimothyNo ratings yet
- Drugs Used in Myocardial InfarctionDocument53 pagesDrugs Used in Myocardial InfarctionSandeep KannegantiNo ratings yet
- Antianginal Student222Document69 pagesAntianginal Student222MoonAIRNo ratings yet
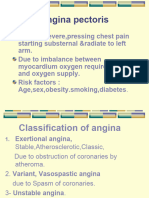
- Angina PectorisDocument11 pagesAngina Pectorisjialin80% (5)
- Antianginal and Antiischemic DrugsDocument18 pagesAntianginal and Antiischemic DrugsNaveen KumarNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisAshwin Raghav SankarNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisAyu PurbaNo ratings yet
- Cardiac DrugsDocument21 pagesCardiac DrugsMona MahfouzNo ratings yet
- Care of Clients With Cardiovascular DisordersDocument67 pagesCare of Clients With Cardiovascular DisordersMatt Lao DionelaNo ratings yet
- Problem 2Document9 pagesProblem 2Chan Myae NaingNo ratings yet
- Case AnalysisDocument5 pagesCase AnalysisCharm TanyaNo ratings yet
- Pharmacology AnginaDocument28 pagesPharmacology AnginaalijanmarwatNo ratings yet
- Anti Anginal DrugsDocument26 pagesAnti Anginal DrugsAtharva PuranikNo ratings yet
- Acute Coronary SyndromesDocument15 pagesAcute Coronary SyndromesAnonymous noiextpGNo ratings yet
- Anti Angina: - Prof. Dr. Rer. Nat. Marianti A. Manggau, AptDocument20 pagesAnti Angina: - Prof. Dr. Rer. Nat. Marianti A. Manggau, Aptwardatnrt12No ratings yet
- Tutorial Antianginal DrugsDocument2 pagesTutorial Antianginal DrugsAbdul MosheenNo ratings yet
- Drugs of CvsDocument32 pagesDrugs of CvsAgus HaryantoNo ratings yet
- Ischemic Heart DiseaseDocument31 pagesIschemic Heart DiseaseRohit SahNo ratings yet
- Antianginal Drugs: Claro M. Isidro M.DDocument34 pagesAntianginal Drugs: Claro M. Isidro M.DNikki ChauhanNo ratings yet
- Inotropes in Cardiothoracic SurgeryDocument44 pagesInotropes in Cardiothoracic SurgeryMarce8118100% (1)
- Medically Compromised PatientDocument32 pagesMedically Compromised Patientمحمد عبدالهادي إسماعيلNo ratings yet
- BPJ 39 Angina Pages 38-47Document10 pagesBPJ 39 Angina Pages 38-47ger4ld1nNo ratings yet
- Pharmacotherapy of Myocardial InfaractionDocument69 pagesPharmacotherapy of Myocardial InfaractionNikhil KamdiNo ratings yet
- Unit 4 Coronary Artery Disease and Ischaemic Heart Disease: StructureDocument37 pagesUnit 4 Coronary Artery Disease and Ischaemic Heart Disease: StructurebtaleraNo ratings yet
- PrelimsDocument11 pagesPrelimsJess Fabra100% (1)
- Medical Management 3 Objectives of ManagementDocument4 pagesMedical Management 3 Objectives of ManagementSaima Sawal SalicNo ratings yet
- Antianginal Drugs.. Prof. Dr. Adeeb Al-ZubaidyDocument19 pagesAntianginal Drugs.. Prof. Dr. Adeeb Al-ZubaidySara AbbasNo ratings yet
- Drugs That Affect The Cardiovascular: Diana Rose D. EmerencianaDocument66 pagesDrugs That Affect The Cardiovascular: Diana Rose D. Emerencianabergonioj511No ratings yet
- Learning Objectives: 1. Relationship Between High Blood Glucose and HyperlipidemiaDocument12 pagesLearning Objectives: 1. Relationship Between High Blood Glucose and HyperlipidemiaDiedreNo ratings yet
- Antianginal Drugs Lecture NotesDocument10 pagesAntianginal Drugs Lecture NotesPrincewill SeiyefaNo ratings yet
- Cardiovacular DisordersDocument7 pagesCardiovacular DisordersAbo AmgadNo ratings yet
- Cad Sihd 2Document67 pagesCad Sihd 2mohammedghassan53No ratings yet
- RNPIDEA-Coronary Artery Disease Nursing Care PlanDocument8 pagesRNPIDEA-Coronary Artery Disease Nursing Care PlanAngie MandeoyaNo ratings yet
- Angina PectorisDocument17 pagesAngina PectorisRacel HernandezNo ratings yet
- Anti - Anginal MedicationDocument41 pagesAnti - Anginal MedicationShine StephenNo ratings yet
- NCP CADDocument31 pagesNCP CADjan100% (1)
- Pharmacology For Nurses: The Islamic UniversityDocument118 pagesPharmacology For Nurses: The Islamic UniversityRojina AdhikariNo ratings yet
- 1.CVS DrugsDocument98 pages1.CVS DrugsHarshika KDGNo ratings yet
- IHD AnginaDocument3 pagesIHD Anginadidaryadgar099No ratings yet
- III) Pharmacotherapy of Angina PectorisDocument23 pagesIII) Pharmacotherapy of Angina PectorisAyro Business CenterNo ratings yet
- Treatment GuidelinesDocument223 pagesTreatment Guidelines14568586794683% (6)
- Ischemic Heart Diease PDFDocument33 pagesIschemic Heart Diease PDFMahamed Wefkey OmranNo ratings yet
- CardiovascularDocument24 pagesCardiovascularAbobakr AlobeidNo ratings yet
- Nursing DiagnosisDocument58 pagesNursing DiagnosisPrecious Santayana100% (3)
- Management of The Patients WithDocument68 pagesManagement of The Patients WithДіна ШоріковаNo ratings yet
- Module 3.3 - CardioDocument12 pagesModule 3.3 - CardioCatherine Sinen ObinqueNo ratings yet
- StrokeDocument22 pagesStrokeAlex GasnasNo ratings yet
- 8 Chapter AnethesiaDocument23 pages8 Chapter AnethesialeonNo ratings yet
- Cardiovascular Diseases 2Document40 pagesCardiovascular Diseases 2Ali MuradNo ratings yet
- Anti Anginal DrugsDocument26 pagesAnti Anginal DrugsAsif Ali LashariNo ratings yet
- Antianginal Drugs DR Hussam 2023Document12 pagesAntianginal Drugs DR Hussam 2023ManWol JangNo ratings yet
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Addison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAddison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Aspek Perpajakan Dalam Transfer Pricing: Related PapersDocument15 pagesAspek Perpajakan Dalam Transfer Pricing: Related PapersHasrawati AzisNo ratings yet
- ProbDocument10 pagesProbKashif JawaidNo ratings yet
- Heirs of Vinluan Estate in Pangasinan Charged With Tax Evasion For Unsettled Inheritance Tax CaseDocument2 pagesHeirs of Vinluan Estate in Pangasinan Charged With Tax Evasion For Unsettled Inheritance Tax CaseAlvin Dela CruzNo ratings yet
- Donnan Membrane EquilibriaDocument37 pagesDonnan Membrane EquilibriamukeshNo ratings yet
- EmployWise JAVA ASSIGNMENTDocument2 pagesEmployWise JAVA ASSIGNMENTPreet PatelNo ratings yet
- Lakh Only) Being The Amount Covered Under The Aforesaid Dishonoured Cheque, and So AlsoDocument2 pagesLakh Only) Being The Amount Covered Under The Aforesaid Dishonoured Cheque, and So AlsoShivam MishraNo ratings yet
- Managemant PrincipleDocument11 pagesManagemant PrincipleEthan ChorNo ratings yet
- 2 - Sample Kids Can Read and Write 2 and 3 Letter Words - Step 2 Final Downloadable Version For Website PDFDocument18 pages2 - Sample Kids Can Read and Write 2 and 3 Letter Words - Step 2 Final Downloadable Version For Website PDFsantoshiNo ratings yet
- Reproduction in PlantsDocument12 pagesReproduction in PlantsAnand Philip PrasadNo ratings yet
- Case Study On Goodearth Financial Services LTDDocument15 pagesCase Study On Goodearth Financial Services LTDEkta Luciferisious Sharma0% (1)
- Heart Rate Variability Threshold As An Alternative.25Document6 pagesHeart Rate Variability Threshold As An Alternative.25Wasly SilvaNo ratings yet
- Islamiyat ProjectDocument21 pagesIslamiyat ProjectSubhan Khan NiaziNo ratings yet
- What Is Denim? Why It's Called Denim?: Properties of Denim FabricDocument21 pagesWhat Is Denim? Why It's Called Denim?: Properties of Denim Fabricrahmanshanto623100% (1)
- Durability of Prestressed Concrete StructuresDocument12 pagesDurability of Prestressed Concrete StructuresMadura JobsNo ratings yet
- VerificationManual en PDFDocument621 pagesVerificationManual en PDFurdanetanpNo ratings yet
- ArrowrootDocument8 pagesArrowrootSevi CameroNo ratings yet
- Dash 3000/4000 Patient Monitor: Service ManualDocument292 pagesDash 3000/4000 Patient Monitor: Service ManualYair CarreraNo ratings yet
- CH 15Document58 pagesCH 15Chala1989No ratings yet
- Atom SDDocument5 pagesAtom SDatomsa shiferaNo ratings yet
- Design Practical Eden Swithenbank Graded PeDocument7 pagesDesign Practical Eden Swithenbank Graded Peapi-429329398No ratings yet
- Bathinda - Wikipedia, The Free EncyclopediaDocument4 pagesBathinda - Wikipedia, The Free EncyclopediaBhuwan GargNo ratings yet
- Ice 3101: Modern Control THEORY (3 1 0 4) : State Space AnalysisDocument15 pagesIce 3101: Modern Control THEORY (3 1 0 4) : State Space AnalysisBipin KrishnaNo ratings yet
- Physico-Chemical Properties of Nutmeg (Myristica Fragrans Houtt) of North Sulawesi NutmegDocument9 pagesPhysico-Chemical Properties of Nutmeg (Myristica Fragrans Houtt) of North Sulawesi NutmegZyuha AiniiNo ratings yet
- Zigbee Technology:19-3-2010: Seminor Title DateDocument21 pagesZigbee Technology:19-3-2010: Seminor Title Dateitdep_gpcet7225No ratings yet
- MSC ACFN2 RD4 ClassDocument25 pagesMSC ACFN2 RD4 Classmengistu jiloNo ratings yet
- Jota - EtchDocument3 pagesJota - EtchRidwan BaharumNo ratings yet
- FDD Spindle Motor Driver: BA6477FSDocument12 pagesFDD Spindle Motor Driver: BA6477FSismyorulmazNo ratings yet
- Vintage Airplane - May 1982Document24 pagesVintage Airplane - May 1982Aviation/Space History LibraryNo ratings yet