You might also like
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Behranwala Et Al. - 2005 - Inflammatory Myofibroblastic Tumour of The Gallbladder-AnnotatedDocument6 pagesBehranwala Et Al. - 2005 - Inflammatory Myofibroblastic Tumour of The Gallbladder-AnnotatedyoussefandabenNo ratings yet
- Primary Ameloblastic Carcinoma of The Maxilla A CaDocument9 pagesPrimary Ameloblastic Carcinoma of The Maxilla A CaMuhammad Avicenna AdjiNo ratings yet
- Ameloblastic Fibrosarcoma or Odontogenic Carcinosarcoma: A Matter of Classification?Document6 pagesAmeloblastic Fibrosarcoma or Odontogenic Carcinosarcoma: A Matter of Classification?Jeyachandran MariappanNo ratings yet
- Inflammatory Myofibroblastic TumourDocument4 pagesInflammatory Myofibroblastic TumourThiruNo ratings yet
- Ajol File Journals - 449 - Articles - 116044 - Submission - Proof - 116044 5329 322635 1 10 20150421Document6 pagesAjol File Journals - 449 - Articles - 116044 - Submission - Proof - 116044 5329 322635 1 10 20150421valeria navarroNo ratings yet
- Art 1Document15 pagesArt 1Nizam Ul MulkNo ratings yet
- Juvenile Ossifying Fibroma of The Mandible: A Case ReportDocument7 pagesJuvenile Ossifying Fibroma of The Mandible: A Case Reportsagarjangam123No ratings yet
- Lucivero Et Al 2011 Lupus Mastitis in Systemic Lupus Erythematosus A Rare Condition Requiring A Minimally InvasiveDocument5 pagesLucivero Et Al 2011 Lupus Mastitis in Systemic Lupus Erythematosus A Rare Condition Requiring A Minimally Invasiveruthdaniel6041No ratings yet
- Inflammatory Myofibroblastic Tumors in The Peculiar Context of The Postpartum Case ReportDocument5 pagesInflammatory Myofibroblastic Tumors in The Peculiar Context of The Postpartum Case ReportIJAR JOURNALNo ratings yet
- Local Anesthetic Thoracoscopy For The Diagnosis of Metastatic Pleural Melanoma Originated From Oral Malignant Melanoma: Case Report and CommentsDocument6 pagesLocal Anesthetic Thoracoscopy For The Diagnosis of Metastatic Pleural Melanoma Originated From Oral Malignant Melanoma: Case Report and CommentsFikri AlfarisyiNo ratings yet
- CRTC1 Ca MucoEpider 10Document6 pagesCRTC1 Ca MucoEpider 10DanielaNo ratings yet
- Malignant Mesothelioma Presenting With Unexplained Recurrent Pleurisy EpisodesDocument4 pagesMalignant Mesothelioma Presenting With Unexplained Recurrent Pleurisy EpisodesNurul NingrumNo ratings yet
- Epithelioid Sarcoma of The Big Toe: A Case ReportDocument4 pagesEpithelioid Sarcoma of The Big Toe: A Case ReportIlincaNo ratings yet
- Recurrence of Mycosis Fungoides On Multiple Melanocytic Nevi: A Case Report and Review of The LiteratureDocument6 pagesRecurrence of Mycosis Fungoides On Multiple Melanocytic Nevi: A Case Report and Review of The LiteraturenanonanditoNo ratings yet
- Myeloma MultipleDocument7 pagesMyeloma MultipleCriissthiiann HernnandezNo ratings yet
- tmpBAE8 TMPDocument6 pagestmpBAE8 TMPFrontiersNo ratings yet
- Varied Presentations of Inverted Papilloma: Case ReportDocument4 pagesVaried Presentations of Inverted Papilloma: Case ReportMohankummar MuniandyNo ratings yet
- Pi Is 0278239103007407Document5 pagesPi Is 0278239103007407tengoplatita2008No ratings yet
- Extracranial Metastases of Anaplastic Meningioma: Case ReportDocument6 pagesExtracranial Metastases of Anaplastic Meningioma: Case ReportRizky AdriansahNo ratings yet
- Long Survival With Metastatic Clear Cell Sarcoma of The Achilles Tendon JFAS 1996Document5 pagesLong Survival With Metastatic Clear Cell Sarcoma of The Achilles Tendon JFAS 1996Evan BowlesNo ratings yet
- Surgical Ciliated Cyst of The Maxilla. Clinical Case: Jorge Cano, Julián Campo, Miguel Angel Alobera, Rafael BacaDocument4 pagesSurgical Ciliated Cyst of The Maxilla. Clinical Case: Jorge Cano, Julián Campo, Miguel Angel Alobera, Rafael BacaAhmad MustafaNo ratings yet
- Abdominal Wall Extraskeletal Ewing Sarcoma - Case ReportDocument3 pagesAbdominal Wall Extraskeletal Ewing Sarcoma - Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- CEOTDocument8 pagesCEOTDrSahar PakzadNo ratings yet
- Gingival and Submandibular Lymph Node Metastasis of Sigmoid Colon AdenocarcinomaDocument4 pagesGingival and Submandibular Lymph Node Metastasis of Sigmoid Colon AdenocarcinomafitriahendricoNo ratings yet
- Stomeo 2009Document5 pagesStomeo 2009elvirNo ratings yet
- CarcinomaDocument5 pagesCarcinomaLori SimmonsNo ratings yet
- Odontogenic Myxoma in A Child: Diagnostic and Treatment DilemmasDocument5 pagesOdontogenic Myxoma in A Child: Diagnostic and Treatment DilemmasthedocperuNo ratings yet
- A Case Report of Desmoplastic AmeloblastomaDocument5 pagesA Case Report of Desmoplastic AmeloblastomaAndria FadliNo ratings yet
- Jhujanax VvjakxvagxhahgxjaDocument4 pagesJhujanax VvjakxvagxhahgxjafauzanNo ratings yet
- A Case of Maxillary Sinus CarcinomaDocument3 pagesA Case of Maxillary Sinus CarcinomajasmniaNo ratings yet
- PMR 2 1 6Document4 pagesPMR 2 1 6Adrian PermadiNo ratings yet
- Mixoma 9Document4 pagesMixoma 9Nicolás MedinaNo ratings yet
- Medicina 60 00066Document8 pagesMedicina 60 00066Thái BìnhNo ratings yet
- Namin 2005Document4 pagesNamin 2005Mohammed FaroukNo ratings yet
- Desdierencia Entre TFS y Glandula ParotidaDocument7 pagesDesdierencia Entre TFS y Glandula ParotidaReyes Ivan García CuevasNo ratings yet
- Inflammatory Conditions Mimicking Tumours in Calabar: A 30 Year Study (1978-2007)Document7 pagesInflammatory Conditions Mimicking Tumours in Calabar: A 30 Year Study (1978-2007)International Organization of Scientific Research (IOSR)No ratings yet
- C CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TDocument7 pagesC CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TG Virucha Meivila IINo ratings yet
- Diagnostic and Therapeutic Pieges Before Clinicoradiological Elements Eviding A Mandibular AmeloblastomaDocument4 pagesDiagnostic and Therapeutic Pieges Before Clinicoradiological Elements Eviding A Mandibular AmeloblastomaAnjay MabarNo ratings yet
- Adenoid Cystic Carcinoma of The Oral CavityDocument5 pagesAdenoid Cystic Carcinoma of The Oral CavityshokoNo ratings yet
- Solitary Fibrous Tumor of Parotid Gland 2022Document6 pagesSolitary Fibrous Tumor of Parotid Gland 2022Reyes Ivan García CuevasNo ratings yet
- Reporte de Casos de MixomaDocument8 pagesReporte de Casos de Mixomacirugia.maxilo.melendezNo ratings yet
- Follow UpDocument6 pagesFollow UpWinda HaeriyokoNo ratings yet
- Li Tiejun2006Document8 pagesLi Tiejun2006Herpika DianaNo ratings yet
- Proptosis UnilateralDocument5 pagesProptosis UnilateralCarlos NiveloNo ratings yet
- Primary Osteosarcoma of The Nasal Fossa: An Exceptional PresentationDocument5 pagesPrimary Osteosarcoma of The Nasal Fossa: An Exceptional PresentationRian HasniNo ratings yet
- Unusual Presentation of Adamantinoma With Synchronous 2024 International JouDocument5 pagesUnusual Presentation of Adamantinoma With Synchronous 2024 International JouRonald QuezadaNo ratings yet
- Wide Field of Cancerization Case Report: February 2017Document5 pagesWide Field of Cancerization Case Report: February 2017Mira AnggrianiNo ratings yet
- Case Report: Palatal Swelling: A Diagnostic EnigmaDocument6 pagesCase Report: Palatal Swelling: A Diagnostic EnigmaPrince AhmedNo ratings yet
- Articulo de Serie de CasoDocument8 pagesArticulo de Serie de CasoJairo Lino BNo ratings yet
- Giant CellDocument5 pagesGiant CellTamimahNo ratings yet
- Adenoma 2020Document11 pagesAdenoma 2020Residentes AudiologiaNo ratings yet
- Adenoid Cystic Carcinoma of Hard Palate: A Case ReportDocument5 pagesAdenoid Cystic Carcinoma of Hard Palate: A Case ReportHemant GuptaNo ratings yet
- Lucrare Stiintifica ParodontologieDocument4 pagesLucrare Stiintifica ParodontologieReduceriAvonNo ratings yet
- Title: Latent Primary Papillary Micro Tumor in Thyroglossal Duct Cyst Wall - A Rare Case Report With Review of LiteratureDocument9 pagesTitle: Latent Primary Papillary Micro Tumor in Thyroglossal Duct Cyst Wall - A Rare Case Report With Review of LiteratureRathinaKumarNo ratings yet
- Extra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalDocument5 pagesExtra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalRonald QuezadaNo ratings yet
- A Case Report of Eumycetoma Early DX CaseDocument3 pagesA Case Report of Eumycetoma Early DX CasesiskaNo ratings yet
- Unicystic Ameloblastoma: A Diagnostic Dilemma and Its Management Using Free Fibula Graft: An Unusual Case ReportDocument4 pagesUnicystic Ameloblastoma: A Diagnostic Dilemma and Its Management Using Free Fibula Graft: An Unusual Case ReportCah YaniNo ratings yet
- Central Giant Cell Granuloma A Case ReportDocument5 pagesCentral Giant Cell Granuloma A Case ReportYara Arafat NueratNo ratings yet
- 115053-Article Text-320504-1-10-20150401Document4 pages115053-Article Text-320504-1-10-20150401AbinayaBNo ratings yet
- Park HydroxyProline 2005jcc PDFDocument5 pagesPark HydroxyProline 2005jcc PDFAngga Witra NandaNo ratings yet
- 1 Bowel Preparation Guidelines FNDocument3 pages1 Bowel Preparation Guidelines FNAngga Witra NandaNo ratings yet
- Park HydroxyProline 2005jcc PDFDocument5 pagesPark HydroxyProline 2005jcc PDFAngga Witra NandaNo ratings yet
- Jgo 27 E1Document10 pagesJgo 27 E1Angga Witra NandaNo ratings yet
- Mak 008 BulDocument4 pagesMak 008 BulAngga Witra NandaNo ratings yet
- CollagenDocument4 pagesCollagenAngga Witra NandaNo ratings yet
- Resecting Branchial Cysts, Fistulae and SinusesDocument13 pagesResecting Branchial Cysts, Fistulae and SinusesAngga Witra NandaNo ratings yet
- Pone 0138000Document12 pagesPone 0138000Angga Witra NandaNo ratings yet
- Park HydroxyProline 2005jcc PDFDocument5 pagesPark HydroxyProline 2005jcc PDFAngga Witra NandaNo ratings yet
- The Evolution of Bowel Preparation and New DevelopDocument8 pagesThe Evolution of Bowel Preparation and New DevelopAngga Witra NandaNo ratings yet
- 2984 7531 1 PBDocument1 page2984 7531 1 PBAngga Witra NandaNo ratings yet
- Whats NewDocument2 pagesWhats NewPanama01No ratings yet
- 09Document5 pages09Angga Witra NandaNo ratings yet
- OperasiDocument35 pagesOperasiAngga Witra NandaNo ratings yet
- Investigation and Management of Obstructive Jaundice PDFDocument7 pagesInvestigation and Management of Obstructive Jaundice PDFAngga Witra NandaNo ratings yet
- Frey Syndrome Complicating Parotidectomy: A Case Report and Review of LiteratureDocument2 pagesFrey Syndrome Complicating Parotidectomy: A Case Report and Review of LiteratureAngga Witra NandaNo ratings yet
- S0022346813X00144 S0022346813008415 MainDocument4 pagesS0022346813X00144 S0022346813008415 MainAngga Witra NandaNo ratings yet
- Proof JOMSDocument11 pagesProof JOMSAngga Witra NandaNo ratings yet
- Bowel InjuryDocument48 pagesBowel InjuryAngga Witra NandaNo ratings yet
- 24 Olsen Variations ParotidectomyDocument33 pages24 Olsen Variations ParotidectomyAngga Witra NandaNo ratings yet
- Fahim VohraDocument7 pagesFahim VohraAchmad Zam Zam AghazyNo ratings yet
- DdlogDocument33 pagesDdlogAngga Witra NandaNo ratings yet
- 9161 BrcicDocument3 pages9161 BrcicAngga Witra NandaNo ratings yet
- Hemolytic Transfusion ReactionDocument3 pagesHemolytic Transfusion ReactionAinin SofiyaNo ratings yet
- Self FlowDocument15 pagesSelf FlowariNo ratings yet
- Diagnostic Imaging - 11 - Regional Pathologies and Evaluation - Shoulder - Elbow - Wrist - Hand - Prof - Dr.i̇smet TAMERDocument34 pagesDiagnostic Imaging - 11 - Regional Pathologies and Evaluation - Shoulder - Elbow - Wrist - Hand - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Assessment of AbdomenDocument99 pagesAssessment of AbdomenKeid ReumaNo ratings yet
- Control and CoordinationDocument15 pagesControl and CoordinationHARSH AKSHIT (B15CS018)No ratings yet
- Trigeminal Nerve VDocument4 pagesTrigeminal Nerve Vm1m2mNo ratings yet
- CHAPTER Respiration and CirculationDocument5 pagesCHAPTER Respiration and CirculationlatasabarikNo ratings yet
- Rev Choi2019 Micromachines 11 00021 v2Document20 pagesRev Choi2019 Micromachines 11 00021 v2Alejandra CastillaNo ratings yet
- Neuroscience: Science of The Brain in NepaliDocument61 pagesNeuroscience: Science of The Brain in NepaliInternational Brain Research Organization100% (1)
- Dictyosome: Modifying, and Packaging Proteins and Lipids Into Vesicles ForDocument11 pagesDictyosome: Modifying, and Packaging Proteins and Lipids Into Vesicles ForASHFAQ AHMAD100% (1)
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- Anatomy and Physiology of The Circulatory SystemDocument7 pagesAnatomy and Physiology of The Circulatory SystemAlessandro Arellano HmuaNo ratings yet
- Medical AstrologyDocument2 pagesMedical Astrologyabhi16No ratings yet
- 11 Biology Notes ch22 Chemical Coordination and Integration PDFDocument6 pages11 Biology Notes ch22 Chemical Coordination and Integration PDFAarav VarshneyNo ratings yet
- Skeletal SystemDocument1 pageSkeletal SystemEzekiel De GuzmanNo ratings yet
- Blood Cell Morphology TutorialDocument176 pagesBlood Cell Morphology TutorialCharles Jebb Belonio JuanitasNo ratings yet
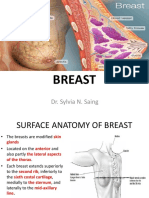
- Breast: Dr. Sylvia N. SaingDocument26 pagesBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- Complete Head-to-Toe Physical Assessment Cheat Sheet: IntegumentDocument8 pagesComplete Head-to-Toe Physical Assessment Cheat Sheet: IntegumentJulianne NeronaNo ratings yet
- PathofBloodFlowHumanBodySystemsCirculatorySystemActivityMSLS13 PDFDocument4 pagesPathofBloodFlowHumanBodySystemsCirculatorySystemActivityMSLS13 PDFOliveenNo ratings yet
- Psychology Canadian 2nd Edition Ciccarelli Test BankDocument25 pagesPsychology Canadian 2nd Edition Ciccarelli Test BankChristopherArnoldoqek100% (38)
- THE FETUS and PLACENTADocument50 pagesTHE FETUS and PLACENTAKyla CalsoNo ratings yet
- Temporomandibular JointDocument28 pagesTemporomandibular JointAli Al-QudsiNo ratings yet
- Urinary System PDFDocument27 pagesUrinary System PDFfiona100% (3)
- Metastatic Vertebral Lesion Mimicking An Atypical Hemangioma WithDocument8 pagesMetastatic Vertebral Lesion Mimicking An Atypical Hemangioma Withsica_17_steaua6519No ratings yet
- Group No. Date Performed Name Date Submitted Facilitator ScoreDocument7 pagesGroup No. Date Performed Name Date Submitted Facilitator ScoreYancy BagsaoNo ratings yet
- Brain ImagesDocument24 pagesBrain Imagesmemoumou27No ratings yet
- Tissue Repair 2016Document16 pagesTissue Repair 2016Luis AndradeNo ratings yet
- Fish Physiology 2Document19 pagesFish Physiology 2Dewi Aisyah TNo ratings yet
- Cells Exploration ActivitiesDocument32 pagesCells Exploration ActivitiesSay KhoNo ratings yet
- Human Circulatory SystemDocument17 pagesHuman Circulatory SystemkangaanushkaNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)