IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 3 Ver. IV (Mar. 2015), PP 24-26
www.iosrjournals.org
Hematoma a life threatening condition: A rare case report
B.M.Rudagi1, Reshma Hammnavar2, Vardan Maheshwari3, Nikunj Patel4
1
Professor Dept of oral and maxillofacial surgery, A C P M dental college Dhule, Maharashtra, India
Senior lecturer Dept of oral and maxillofacial surgery,A C P M dental college Dhule, Maharashtra, India
3
Post graduate student Dept of and maxillofacial surgery A C P M dental college Dhule, Maharashtra, India
4
Post graduate student Dept of oral and maxillofacial surgery,A C P M dental college Dhule, Maharashtra,
India
2
Abstract: Hematoma is a mass of coagulated or extravasated blood in a cavity or closed tissue space. It can
induce many infections if exposed to the exogenous or endogenous pathogens. High risk of infection after
trauma is related to several factors: poor perfusion, shock, tissue viability following necrosis or hemorrhage,
the number and virulence of organisms and host resistance. The presence of hematoma or accumulation of
serum, and devitalisation and ischaemia of injured tissue, provides a favorable environment for growth of
pathogens, including anaerobic bacteria, with decreased access of immune response. In the reported case, the
post traumatic hematoma got infected and the patient developed cellulitis, which spread to the other spaces in
the neck and caused difficulty in airway, speech and mastication. Antibiotics were prescribed to curb the
infection and serratiopeptidase enzyme was administered for the purpose of suppressing and eliminating the
post traumatic bleeding and hematoma. The main objective here was to prevent airway obstruction and avert a
serious, life threatening condition.
Key words- Hematoma, infection, cellulitis, life threatening condition
I. Introduction
Hematoma is a mass of coagulated or extravasated blood in a cavity or closed tissue space. 1It is
localized swelling that is filled with blood caused by a break in the wall of a blood vessel. The breakage may be
spontaneous, as in the case of an aneurysm, or caused by trauma. The word "haematoma" came into usage
around 1850 and is derived from the Greek roots "hemat-" (blood) and -oma, from soma, meaning body = a
body of blood. Another etymological derivation would be from "haemat-" = blood-and "-oma" = "-ing", thus
simply "bleeding". Hematomas form into hard masses under the surface of the skin. This is caused by the
limitation of the blood to a subcutaneous or intramuscular tissue space isolated by fascial planes. This is a key
anatomical feature that prevents such injuries from causing massive blood loss. In most cases the sac of blood or
hematoma eventually dissolves; however, in some cases they may continue to grow or show no change. If the
sac of blood does not disappear, then it may need to be surgically removed.
Injury mechanisms such as falls, assaults, sports injuries, and vehicle crashes are common causes of
facial trauma in children2 as well as in adults. Blunt assault, blows from fists or objects, are a common cause of
facial injury.3 Nearly 10% of patients with craniomaxillofacial fractures sustain intracranial hemorrhages
requiring frequently immediate neurosurgical intervention. Those patients, suffering from central midface
fractures and skull base fractures, are prone to highly significant elevated risks of intracranial hemorrhage. 4
II. Case report
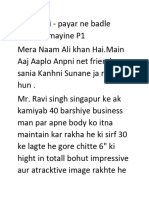
A 10 year old male patient, reported to the department of Oral and Maxillofacial Surgery with swelling
in the right preauricular region, following blunt trauma due to interpersonal violence at school (fig.1). The
patient revealed that the initial swelling was small, and he experienced mild pain over the pre auricular region.
As a result, he neglected the swelling, which, over the next 4 days increased in size. On examination, the
swelling was roughly oval in shape, with ill defined margins, extending from right preauricular and
submandibular regions to cross the midline and reach up to the middle of the neck, superior-inferiorly; and
antero-posteriorly, from the right corner of the mouth to the tragus. The swelling was firm, indurated, woody
hard, non-pitting, non-fluctuant and associated with tenderness and trismus. Crepitations were also felt in the
neck region. The orthopantomograph appeared normal, with no relevant findings. The above findings were
indicative of cellulitis which had spread to the other spaces in the neck and caused difficulty in breathing,
speech and mastication.
A non-surgical, conservative approach was chosen for treatment. An I.V. line was established using
No. 22 veinflow. Patient was administered I.V. antibiotics and steroids with oral doses of analgesics and
antacids. O2 was also administered at the rate of 2-3 litres/ hour for 3 consecutive days. A surgical approach
(incision and drainage) was also planned for decompression of the spaces involved, but the patient responded
DOI: 10.9790/0853-14342426
www.iosrjournals.org
24 | Page
Hematoma a life threatening condition: A rare case report
well to the I.V. antibiotics regimen as prescribed above. The swelling subsided within 3 days and the facial
profile of the patient was back to normal (fig.2).
III. Discussion
Hematoma is a swollen or raised area at the venipuncture site resulting from leakage of blood into the
tissues. The size and spread of a hematoma depends on its vascular origin (capillary, venous or arterial) and the
tissue into which it is bleeding (muscle, fat or interstitia). Hematomas stop expanding when the pressure of the
pooling blood exceeds the vascular pressure of the bleeding site. It can be viewed in three time frames: pre, peri
and postoperative. Although no literature has provided a failsafe set of predictors as to which patients are at risk
and which are not.5 The role of the mandibular fracture hematoma could be as a presumptive local reservoir for
osteogenic progenitors and thus contribute to intramembranous bone healing.6
Classification
Types
Subdermal hematoma (under the skin)
Skull/brain:
Subgaleal hematoma between the galea aponeurosis and periosteum
Cephalohematoma between the periosteum and skull. Commonly caused by vacuum delivery and vertex
delivery.
Epidural hematoma between the skull and dura mater
Subdural hematoma between the dura mater and arachnoid mater
Subarachnoid hematoma between the arachnoid mater and pia mater (the subarachnoid space)
Othematoma between the skin and the layers of cartilage of the ear
Perichondral hematoma (ear)
Perianal hematoma (anus)
Subungual hematoma (nail)
Degrees
Petechiae small pinpoint hematomas less than 3 mm in diameter
Purpura (purple) a bruise about 1 cm in diameter, generally round in shape
Ecchymosis subcutaneous extravasation of blood in a thin layer under the skin, i.e. bruising or "black and
blue," over 1 cm in diameter
Trauma often leads to inflammatory responses which induces the release of numerous vasoactive
angiogenic pyrogens, which produce vasodilatation within a few hours of injury.7 Hemorrhage from the dilated,
damaged vessels of the endosteum, periosteum and Haversian system leads to hematoma formation. 8 Hematoma
can induce many infections if exposed to the exogenous or endogenous pathogens. 9 Most previous reports of
infection after trauma in children have highlighted the importance of aerobic or facultative organisms. 10
High risk of infection after trauma is related to several factors: poor perfusion, shock, tissue viability
following necrosis or hemorrhage, the number and virulence of organisms and host resistance .11 The presence
of hematoma or accumulation of serum, and devitalisation and ischaemia of injured tissue, provides a favorable
environment for growth of pathogens, including anaerobic bacteria, with decreased access of immune response.9
An etiologic diagnosis of simple cellulitis is frequently difficult, and generally unnecessary for patients
with mild signs and symptoms of illness. Clinical assessment of the severity of infection is crucial, and several
classification schemes and algorithms have been proposed to guide the clinician. 12 Hematomas of skin and soft
tissues are often treated with RICE (rest, ice, compression, elevation). Emerging antibiotic resistance among
Staphylococcus aureus (Methicillin resistance) and Streptococcus pyogenes (Erythromycin resistance) are
problematic, because both of these organisms are common causes of a variety of skin and soft-tissue infections;
and because empirical choices of antimicrobials must include agents with activity against resistant strains.
Minor skin and soft-tissue infections may be empirically treated with semi-synthetic Penicillin, First-generation
or Second-generation oral Cephalosporins, Macrolides, or Clindamycin. It is prudent to re-evaluate them in 24
48 hours to verify a clinical response. However surgical decompression combined with drainage enables
complete evacuation of the blood clot and prevents possible sequelae. 13
In the reported case, the post traumatic hematoma got infected and the patient developed cellulitis,
which spread to the other spaces in the neck and caused difficulty in airway, speech and mastication. Antibiotics
were prescribed to curb the infection and serratiopeptidase enzyme was administered for the purpose of
suppressing and eliminating the post traumatic bleeding and hematoma. The main objective here was to prevent
DOI: 10.9790/0853-14342426
www.iosrjournals.org
25 | Page
Hematoma a life threatening condition: A rare case report
airway obstruction and avert a serious, life threatening condition. Incision and drainage was the alternative
treatment of choice.
IV. Conclusion
A case of post traumatic infected hematoma has been presented. We have discussed the clinical
implications of a diagnosis of hematoma, its consequences and management. The surgeon plays crucial roles in
recognizing and managing many emergencies. The most immediate danger for this swelling which started as a
small, mild painful swelling in the preauricular region and due to negligence by the patient got infected and
lead to cellulitis stage crossing the midline. Active measures should be taken to secure the airway and
administering the proper antibiotics so that the emergency can be managed appropriately.
Fig.1 Pre hospitalization photographs
Fig. 2 Discharge photo
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
Miller SJ: "Edema, Hematoma, and lnfection," in McGlamry, ED (ed) Comprehensive Textbook of Foot Surgery,Williams &
Wilkins, Baltimore, Maryland, 1 0l 5, 1031 , 1034, 1987.
Neuman MI, Eriksson E (2006). "Facial trauma". In Fleisher GR, Ludwig S, Henretig FM. Textbook of Pediatric Emergency
Medicine. Hagerstwon, MD: Lippincott Williams & Wilkins. Retrieved 2008-10-19.
Seyfer AE, Hansen JE (2003). "Facial trauma". In Moore EE, Feliciano DV, Mattox KL. Trauma. Fifth Edition. McGraw-Hill
Professional. pp. 42324.
M Hohlrieder, J Hinterhoelzl, H Ulmer, W Hackl, E Schmutzhard, R Gassner Maxillofacial fractures masking traumatic intracranial
hemorrhages. International journal of oral and maxillofacial surgery 2004; 33: 389-394.
Rees TD, Lee YC, Couburn RJ. Expanding hematoma after rhytidectomy: a retrospective study. Plast Reconstr Surg 1973;51:14953.
Takumi Hasegawa, Masahiko Miwa, Yoshitada Sakai, Takahiro Nikura, Sang Yang Lee, Keisuke Oe, Takashi Iwakura, Masahiro
Kurosaka, Takahide Komori Mandibular hematoma cells as a potential reservior for osteoprogenitor cells in fracture. Journal of oral
and maxillofacial surgery, 2012; 70: 599-607
Simmons DJ: fracture healing. In Urist MR (ed) : Fundamental and clinical bone physiology. Philadelphia, JB Lippincott, 1980, pp
283-330.
Simmons DJ: Fracture healing perspectives. Clin Orthop Rel Res 200:100.1985.
Itzhak Brook aerobic and anerobic microbiology of infection after trauma in children J. Accid Emerg Med 1998;15:162-67.
Nichols RL, Smith JW. Gas in the wound: what does it mean? Surg Clin North Am 1975;55:1289-96.
Caplan ES, Hoyt N infection survillence and control in the severely traumatized patient. In dixon J, ed , nosocomial infectios,, n ew
York: yorke medical book, 1982;247-51.
Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory risk indicator for necr otizing fasciitis) score: a tool
for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med 2004; 32:153541.
Dinko Leovic, Vedran Zubcic, Mirta Kopic, Marko Matijevic, Davorin Danic post traumatic subperiosteal orbital hematoma.
Journal of cranio-maxillofacial surgery 2011; 39: 131-134.
DOI: 10.9790/0853-14342426
www.iosrjournals.org
26 | Page
You might also like
- Study The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueDocument9 pagesStudy The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueInternational Organization of Scientific Research (IOSR)No ratings yet
- Philosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemDocument6 pagesPhilosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemInternational Organization of Scientific Research (IOSR)No ratings yet
- Students' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaDocument6 pagesStudents' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaInternational Organization of Scientific Research (IOSR)No ratings yet
- Necessary Evils of Private Tuition: A Case StudyDocument6 pagesNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)No ratings yet
- Project Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachDocument5 pagesProject Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachInternational Organization of Scientific Research (IOSR)No ratings yet
- The Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)Document11 pagesThe Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)International Organization of Scientific Research (IOSR)No ratings yet
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDocument10 pagesEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Enhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemDocument7 pagesEnhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemInternational Organization of Scientific Research (IOSR)No ratings yet
- Development of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationDocument5 pagesDevelopment of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationInternational Organization of Scientific Research (IOSR)No ratings yet
- Geohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesDocument14 pagesGeohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesInternational Organization of Scientific Research (IOSR)No ratings yet
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDocument5 pagesYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Need of Non - Technical Content in Engineering EducationDocument3 pagesNeed of Non - Technical Content in Engineering EducationInternational Organization of Scientific Research (IOSR)No ratings yet
- Child Mortality Among Teenage Mothers in OJU MetropolisDocument6 pagesChild Mortality Among Teenage Mothers in OJU MetropolisInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurDocument4 pagesComparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurInternational Organization of Scientific Research (IOSR)No ratings yet
- Lipoproteins and Lipid Peroxidation in Thyroid DisordersDocument6 pagesLipoproteins and Lipid Peroxidation in Thyroid DisordersInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoDocument2 pagesComparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoInternational Organization of Scientific Research (IOSR)No ratings yet
- Microencapsulation For Textile FinishingDocument4 pagesMicroencapsulation For Textile FinishingInternational Organization of Scientific Research (IOSR)No ratings yet
- Study of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyDocument9 pagesStudy of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyInternational Organization of Scientific Research (IOSR)No ratings yet
- Core Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseDocument5 pagesCore Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDocument2 pagesComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)No ratings yet
- Advancing Statistical Education Using Technology and Mobile DevicesDocument9 pagesAdvancing Statistical Education Using Technology and Mobile DevicesInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsDocument6 pagesComparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsInternational Organization of Scientific Research (IOSR)No ratings yet
- Application of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelDocument8 pagesApplication of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelInternational Organization of Scientific Research (IOSR)No ratings yet
- Auxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaDocument4 pagesAuxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaInternational Organization of Scientific Research (IOSR)No ratings yet
- A Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentDocument4 pagesA Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentInternational Organization of Scientific Research (IOSR)No ratings yet
- Investigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeDocument5 pagesInvestigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeInternational Organization of Scientific Research (IOSR)No ratings yet
- Factors Affecting Success of Construction ProjectDocument10 pagesFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)No ratings yet
- Research Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaDocument7 pagesResearch Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Parametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendDocument6 pagesParametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendInternational Organization of Scientific Research (IOSR)No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Biologically Active Compounds From Hops and Prospects For Their Use - Karabín 2016Document26 pagesBiologically Active Compounds From Hops and Prospects For Their Use - Karabín 2016Micheli Legemann MonteNo ratings yet
- By This Axe I Rule!Document15 pagesBy This Axe I Rule!storm0% (1)
- Method Statement For Cable Trays & Cable Ladders InstallationDocument7 pagesMethod Statement For Cable Trays & Cable Ladders InstallationJamal Budeiri0% (1)
- Sketchup-Rhino Cheat SheetDocument1 pageSketchup-Rhino Cheat Sheetxanext7No ratings yet
- Leadership Games and ActivitiesDocument38 pagesLeadership Games and ActivitiesWilliam Oliss100% (1)
- Comparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanDocument4 pagesComparative Performance of Some Cattle Breeds Under Barani Conditions of PakistanMasood HassanNo ratings yet
- 4 5803133100506483687Document245 pages4 5803133100506483687Malik HamidNo ratings yet
- Salapare Et Al 2015 ZambalesDocument12 pagesSalapare Et Al 2015 ZambalesTiqfar AhmadjayadiNo ratings yet
- Industrial Internet of Things: Presented To-Presented byDocument18 pagesIndustrial Internet of Things: Presented To-Presented byGaurav RaturiNo ratings yet
- Class 12 - Maths - MatricesDocument87 pagesClass 12 - Maths - MatricesAishwarya MishraNo ratings yet
- Salem RPGDocument16 pagesSalem RPGabstockingNo ratings yet
- SPM 1449 2006 Mathematics p2 BerjawapanDocument18 pagesSPM 1449 2006 Mathematics p2 Berjawapanpss smk selandar71% (7)
- GLP BmsDocument18 pagesGLP BmsDr.Subhashish TripathyNo ratings yet
- Chapter 04 Product and ServDocument43 pagesChapter 04 Product and ServAlireza AlborziNo ratings yet
- Accsap 10 VHDDocument94 pagesAccsap 10 VHDMuhammad Javed Gaba100% (2)
- Properties of Matter ReviewDocument8 pagesProperties of Matter Reviewapi-290100812No ratings yet
- S590 Machine SpecsDocument6 pagesS590 Machine SpecsdilanNo ratings yet
- Communication Guide: For Vita 62 Compliant VPX Power SuppliesDocument8 pagesCommunication Guide: For Vita 62 Compliant VPX Power Suppliesk.saikumarNo ratings yet
- Rac Question PaperDocument84 pagesRac Question PaperibrahimNo ratings yet
- Trends in FoodDocument3 pagesTrends in FoodAliNo ratings yet
- Sheet Metal Manufacturing Companies NoidaDocument9 pagesSheet Metal Manufacturing Companies NoidaAmanda HoldenNo ratings yet
- Angewandte: ChemieDocument13 pagesAngewandte: ChemiemilicaNo ratings yet
- IPC's 2 Edition of Guidance Manual For Herbs and Herbal Products Monographs ReleasedDocument1 pageIPC's 2 Edition of Guidance Manual For Herbs and Herbal Products Monographs ReleasedRakshaNo ratings yet
- Future AncestorsDocument44 pagesFuture AncestorsAlex100% (1)
- Ge Fairchild Brochure PDFDocument2 pagesGe Fairchild Brochure PDFDharmesh patelNo ratings yet
- Differential Geometry of Curves and Surfaces 3. Regular SurfacesDocument16 pagesDifferential Geometry of Curves and Surfaces 3. Regular SurfacesyrodroNo ratings yet
- Uji Efektivitas Mikroba Rumpun BambuDocument7 pagesUji Efektivitas Mikroba Rumpun BambuUse Real ProjectNo ratings yet
- Firestone & Scholl - Cognition Does Not Affect Perception, Evaluating Evidence For Top-Down EffectsDocument77 pagesFirestone & Scholl - Cognition Does Not Affect Perception, Evaluating Evidence For Top-Down EffectsRed JohnNo ratings yet
- Ventricular Septal DefectDocument9 pagesVentricular Septal DefectpepotchNo ratings yet
- Manual Nice9000v A04Document151 pagesManual Nice9000v A04hoang tamNo ratings yet