You might also like
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- Eric Berg CVDocument6 pagesEric Berg CVHaralambicNo ratings yet
- Prometric McqsDocument30 pagesPrometric Mcqsjishan8250% (2)
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Full-Mouth Adhesive Rehabilitation in Case of Severe Dental Erosion, A Minimally Invasive Approach Following The 3-Step TechniqueDocument18 pagesFull-Mouth Adhesive Rehabilitation in Case of Severe Dental Erosion, A Minimally Invasive Approach Following The 3-Step TechniqueHoracio Mendia100% (1)
- Ipsg 6 Patient SafetyDocument12 pagesIpsg 6 Patient SafetyJamilaturRasyidahEfendiNo ratings yet
- Treatment of Cardiac Arrest in The Hyperbaric Environment - Key Steps On The Sequence of Care - Case ReportsDocument8 pagesTreatment of Cardiac Arrest in The Hyperbaric Environment - Key Steps On The Sequence of Care - Case Reportstonylee24No ratings yet
- Patient Perceptions of Emergency Department Fast Track: A Prospective Pilot Study Comparing Two Models of CareDocument3 pagesPatient Perceptions of Emergency Department Fast Track: A Prospective Pilot Study Comparing Two Models of CareErvin WidhiantyasNo ratings yet
- BiblioDocument7 pagesBiblioErikaCacatianNo ratings yet
- Qualitative ResearchDocument9 pagesQualitative ResearchGideon M KimariNo ratings yet
- J 1553-2712 2011 01122 X PDFDocument8 pagesJ 1553-2712 2011 01122 X PDFSriatiNo ratings yet
- 10 1093@intqhc@mzx017 PDFDocument6 pages10 1093@intqhc@mzx017 PDFMeli SariNo ratings yet
- CPG Management of Childhood Asthma (2014)Document20 pagesCPG Management of Childhood Asthma (2014)Haz100% (1)
- Reliability Study of The Rapid Emergency Triage ChildrenDocument6 pagesReliability Study of The Rapid Emergency Triage ChildrentiavmexNo ratings yet
- Endoscopic Skills Training in A Simulated Clinical.8Document6 pagesEndoscopic Skills Training in A Simulated Clinical.8Alberto Kenyo Riofrio PalaciosNo ratings yet
- CNL Role in Reducing ICU EVD InfectionsDocument35 pagesCNL Role in Reducing ICU EVD InfectionsPaolo VegaNo ratings yet
- 422 PaperDocument8 pages422 Paperapi-384505435No ratings yet
- Geriatric Nursing: Canan Karadas, MSC, Leyla Ozdemir, RN, PHDDocument6 pagesGeriatric Nursing: Canan Karadas, MSC, Leyla Ozdemir, RN, PHDCharah IC NuRseNo ratings yet
- Emergency DepartmentDocument9 pagesEmergency DepartmentSarah Mae SanchezNo ratings yet
- Developing Clinical Guidelines for Initial Trauma Patient AssessmentDocument3 pagesDeveloping Clinical Guidelines for Initial Trauma Patient AssessmentErikaCacatianNo ratings yet
- Sact Passport Final Aug 2020Document68 pagesSact Passport Final Aug 2020ryze.ahmedNo ratings yet
- ARCHANA MUKHERJEE Project On Woodlands HospitalDocument26 pagesARCHANA MUKHERJEE Project On Woodlands Hospitaldipannita adhikaryNo ratings yet
- Biblio Ms Abcrisis NCM 107 1Document3 pagesBiblio Ms Abcrisis NCM 107 1Nica SalazarNo ratings yet
- Zhang 2013Document5 pagesZhang 2013Fahmina AkramNo ratings yet
- Critical Care Nurses' Knowledge RegardingManagement of Patients WithAtrial Fibrillation at Baghdad CityDocument5 pagesCritical Care Nurses' Knowledge RegardingManagement of Patients WithAtrial Fibrillation at Baghdad CityIOSRjournalNo ratings yet
- Literature Review Nurse Fatigue Related To Shift LengthDocument4 pagesLiterature Review Nurse Fatigue Related To Shift LengthafmzetkeybbaxaNo ratings yet
- The Effect of An Emergency Department Dedicated Midtrack Area On Patient FlowDocument6 pagesThe Effect of An Emergency Department Dedicated Midtrack Area On Patient FlowBeny HermawanNo ratings yet
- 002 27998am1012s14 13 25Document13 pages002 27998am1012s14 13 25Zainal Abidin Mbah JinonNo ratings yet
- Dyspnea ProjectDocument20 pagesDyspnea Projectfarah.abd97No ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Translating Research Evidence Into Action in Daily PracticeDocument2 pagesTranslating Research Evidence Into Action in Daily PracticesooyoungNo ratings yet
- Safe Sedation PracticeDocument39 pagesSafe Sedation PracticeAlaa ShnienNo ratings yet
- Geriatric Hospital Nurses' Knowledge, Attitude Toward Falls, and Fall Prevention ActivitiesDocument11 pagesGeriatric Hospital Nurses' Knowledge, Attitude Toward Falls, and Fall Prevention Activitieskang soon cheolNo ratings yet
- Songwathana2011 PDFDocument8 pagesSongwathana2011 PDFoh yuniNo ratings yet
- Aew 190Document8 pagesAew 190Nurul Dwi LestariNo ratings yet
- Safe Surgery JournalDocument10 pagesSafe Surgery JournalNur LaelaNo ratings yet
- Viewcontent CgiDocument15 pagesViewcontent CgiasandiNo ratings yet
- Adherence To The Guideline Triage in Emergency Departments' A SurveyDocument12 pagesAdherence To The Guideline Triage in Emergency Departments' A Surveyririnf2165No ratings yet
- Clinical JudgmentDocument6 pagesClinical Judgmentapi-662433822No ratings yet
- Occupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyDocument12 pagesOccupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyIlvita MayasariNo ratings yet
- Effectofcarereducationon Functionalabilitiesofpatients WithstrokeDocument7 pagesEffectofcarereducationon Functionalabilitiesofpatients WithstrokeDan Gerald Alcido SalungaNo ratings yet
- Experienced Physiotherapist ResumeDocument4 pagesExperienced Physiotherapist ResumeAndrew WongNo ratings yet
- Model of International Training of Cardiac SurgeryDocument17 pagesModel of International Training of Cardiac SurgeryMore InterestingNo ratings yet
- R P H I T C T: Educing Atient Andling Njuries Hrough Ontextual RainingDocument5 pagesR P H I T C T: Educing Atient Andling Njuries Hrough Ontextual RainingerryNo ratings yet
- 1 Running Head: Therapeutic Nursing InterventionsDocument8 pages1 Running Head: Therapeutic Nursing Interventionsapi-337126539No ratings yet
- Mila 1Document5 pagesMila 1Milagros SGNo ratings yet
- Tintu Jones Karedan - 121534968Document5 pagesTintu Jones Karedan - 121534968Mumtaj AnsariNo ratings yet
- Chapter 1-3Document27 pagesChapter 1-3JellyAnnGomezNo ratings yet
- First Author 2010 International-Emergency-Nursing 1Document5 pagesFirst Author 2010 International-Emergency-Nursing 1anon_543702124No ratings yet
- Jurnal 8Document7 pagesJurnal 8myra umarNo ratings yet
- Preoperative AssessmentDocument9 pagesPreoperative Assessment1234chocoNo ratings yet
- Sepsis KnowledgeDocument7 pagesSepsis KnowledgeFalah IsmailNo ratings yet
- Ito Et Al-2012-Pediatrics InternationalDocument19 pagesIto Et Al-2012-Pediatrics Internationalakhmad alya maulanaNo ratings yet
- Pre Hospital PDFDocument4 pagesPre Hospital PDFAndi Tri SutrisnoNo ratings yet
- Critical Care Delivery in India: Roles of Consultant IntensivistsDocument28 pagesCritical Care Delivery in India: Roles of Consultant IntensivistsEsther RaniNo ratings yet
- Research Paper On Life SupportDocument7 pagesResearch Paper On Life Supportshvximwhf100% (1)
- Triage PDFDocument7 pagesTriage PDFAnonymous nEQNlgbYQCNo ratings yet
- Article in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudyDocument7 pagesArticle in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudySimson TameonNo ratings yet
- Amira Ali KnowledgeDocument15 pagesAmira Ali KnowledgeMohammed RefaatNo ratings yet
- PA Final Report Jan 09 Version 5Document47 pagesPA Final Report Jan 09 Version 5Sean HalliganNo ratings yet
- NILES-Volume 4-Issue 2 - Page 301-317Document17 pagesNILES-Volume 4-Issue 2 - Page 301-317Maged SaadNo ratings yet
- Evaluating The Quality of Care Delivered by An Emergency Department Fast Track Unit With Both Nurse Practitioners and DoctorsDocument7 pagesEvaluating The Quality of Care Delivered by An Emergency Department Fast Track Unit With Both Nurse Practitioners and DoctorspoppyNo ratings yet
- Australasian Emergency Care: Happy I. Kusumawati, Judy Magarey, Philippa RasmussenDocument6 pagesAustralasian Emergency Care: Happy I. Kusumawati, Judy Magarey, Philippa Rasmussenrida rahmayantiNo ratings yet
- Clinical Nurse Specialist Role and Practice: An International PerspectiveFrom EverandClinical Nurse Specialist Role and Practice: An International PerspectiveJanet S. FultonNo ratings yet
- A Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostDocument6 pagesA Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostIJRASETPublicationsNo ratings yet
- Minimum Inhibitory ConcentrationDocument7 pagesMinimum Inhibitory ConcentrationToshio HamazakiNo ratings yet
- English Intervention DialogueDocument3 pagesEnglish Intervention DialogueJihan Irbah TrianiNo ratings yet
- Basic pharmacology of anaesthesia drugs in 40 charactersDocument56 pagesBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87No ratings yet
- Rheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009Document9 pagesRheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009drwstokes100% (1)
- GROUP 10 Senstive Abt Food and Food AllergiesDocument16 pagesGROUP 10 Senstive Abt Food and Food AllergiesLilis nopita SarryNo ratings yet
- Buletin Farmasi 1/2014Document14 pagesBuletin Farmasi 1/2014afiq83100% (1)
- GetPdf Cgi PDFDocument9 pagesGetPdf Cgi PDFAKNTAI002No ratings yet
- Hypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentDocument11 pagesHypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentAnantaBenvenutoNo ratings yet
- Should Medical Marijuana Be Legalized For PatientsDocument4 pagesShould Medical Marijuana Be Legalized For PatientsBing Cossid Quinones CatzNo ratings yet
- 19 Spinal CordDocument8 pages19 Spinal Cordkarar AhmedNo ratings yet
- Hipertensi Portal Donny SandraDocument67 pagesHipertensi Portal Donny SandrabobyNo ratings yet
- 5a.ESOPHAGEAL DISORDERSDocument16 pages5a.ESOPHAGEAL DISORDERSHayat AL AKOUMNo ratings yet
- Effects of Malnutrition Among ChildrenDocument3 pagesEffects of Malnutrition Among ChildrenDesiree Aranggo MangueraNo ratings yet
- Dementia Incidence, Burden and Cost of Care: A Filipino Community-Based StudyDocument9 pagesDementia Incidence, Burden and Cost of Care: A Filipino Community-Based StudyVanessa PalomaNo ratings yet
- FormsDocument15 pagesFormsBiswajit DasNo ratings yet
- Medical Assessment Form Blank-1Document4 pagesMedical Assessment Form Blank-1Zakiya HassanNo ratings yet
- Volume 43, Number 12, March 23, 2012Document56 pagesVolume 43, Number 12, March 23, 2012BladeNo ratings yet
- Leaflet YTiG Plus Tablet For CHCDocument1 pageLeaflet YTiG Plus Tablet For CHCDesi Health Tips UpdateNo ratings yet
- TimeWise Miracle Set 3D Fact Sheet MYSG ENGDocument2 pagesTimeWise Miracle Set 3D Fact Sheet MYSG ENGKilinSilinNo ratings yet
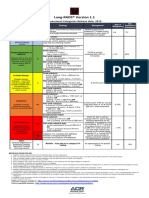
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Sgot & SGPTDocument2 pagesSgot & SGPT우영박No ratings yet
- FOAT Readings and ResourcesDocument1 pageFOAT Readings and Resourcesagnes windramNo ratings yet
- Retrograde Intubation Using Epidural Catheter - A Safe and Cost Effective Technique - A Case ReportDocument2 pagesRetrograde Intubation Using Epidural Catheter - A Safe and Cost Effective Technique - A Case ReportIOSRjournalNo ratings yet
- Global Tuberculosis Report 2018 PDFDocument243 pagesGlobal Tuberculosis Report 2018 PDFDudungNo ratings yet