You might also like
- Hearing Voices: Qualitative Inquiry in Early PsychosisFrom EverandHearing Voices: Qualitative Inquiry in Early PsychosisNo ratings yet
- Pediatric Gender Identity: Gender-affirming Care for Transgender & Gender Diverse YouthFrom EverandPediatric Gender Identity: Gender-affirming Care for Transgender & Gender Diverse YouthMichelle ForcierNo ratings yet
- Cutajar CSA Psychopathology CAN Paper Proof 2010Document10 pagesCutajar CSA Psychopathology CAN Paper Proof 2010Cariotica AnonimaNo ratings yet
- Eating Disorders in Boys and MenFrom EverandEating Disorders in Boys and MenJason M. NagataNo ratings yet
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyFrom EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNo ratings yet
- Pediatric Consultation-Liaison Psychiatry: A Global, Healthcare Systems-Focused, and Problem-Based ApproachFrom EverandPediatric Consultation-Liaison Psychiatry: A Global, Healthcare Systems-Focused, and Problem-Based ApproachAnthony P. S. GuerreroNo ratings yet
- McElroy Et Al. (2016)Document11 pagesMcElroy Et Al. (2016)voooNo ratings yet
- 2014 Baglivio Et Al. The Prevalence of Adverse Childhood Experiences (ACE) in The Lives of Juvenile OffendersDocument23 pages2014 Baglivio Et Al. The Prevalence of Adverse Childhood Experiences (ACE) in The Lives of Juvenile OffenderskakonautaNo ratings yet
- Debriefing SheetDocument5 pagesDebriefing SheetAyuningNo ratings yet
- Adult Survivors Understanding the Long-Term Effects of Traumatic Childhood ExperiencesFrom EverandAdult Survivors Understanding the Long-Term Effects of Traumatic Childhood ExperiencesRating: 5 out of 5 stars5/5 (1)
- Emotional Distress Resilience and Adaptability A Qualitative Study of Adults Who Experienced Infant AbandonmentDocument18 pagesEmotional Distress Resilience and Adaptability A Qualitative Study of Adults Who Experienced Infant AbandonmentLoredana Pirghie AntonNo ratings yet
- Peer Victimization PaperDocument21 pagesPeer Victimization Paperapi-249176612No ratings yet
- 3 Delinquent Mta Molinaetal07Document13 pages3 Delinquent Mta Molinaetal07lucasher35No ratings yet
- Impact of Early Medical Treatment For Transgender Youth: Protocol For The Longitudinal, Observational Trans Youth Care StudyDocument10 pagesImpact of Early Medical Treatment For Transgender Youth: Protocol For The Longitudinal, Observational Trans Youth Care StudycatalinavillenaNo ratings yet
- Diagnosis and Treatment of Children With Autism Spectrum DisordersFrom EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersRating: 5 out of 5 stars5/5 (1)
- PTSD From Childhood Trauma As A PrecursoDocument20 pagesPTSD From Childhood Trauma As A PrecursoDavid QatamadzeNo ratings yet
- RecommendedDocument12 pagesRecommendedMaya Putri HaryantiNo ratings yet
- INFANCIA - Turban (2017) Transgender Youth - The Building Evidence Base For Early Social TransitionDocument2 pagesINFANCIA - Turban (2017) Transgender Youth - The Building Evidence Base For Early Social TransitionMiizhy CakeNo ratings yet
- Child Maltreatment Assessment-Volume 2: Sexual, Emotional, and Psychological AbuseFrom EverandChild Maltreatment Assessment-Volume 2: Sexual, Emotional, and Psychological AbuseNo ratings yet
- Medical Response to Child Sexual Abuse: A Resource for Professionals Working with Children and FamiliesFrom EverandMedical Response to Child Sexual Abuse: A Resource for Professionals Working with Children and FamiliesNo ratings yet
- Analise Sobre Facilitadores e Dificuldades ABSDocument24 pagesAnalise Sobre Facilitadores e Dificuldades ABSMadalena SilvaNo ratings yet
- TMS y OHDocument14 pagesTMS y OHLaura AlfaroNo ratings yet
- Medical Response to Adult Sexual Assault: A Resource for Clinicians and Related ProfessionalsFrom EverandMedical Response to Adult Sexual Assault: A Resource for Clinicians and Related ProfessionalsNo ratings yet
- Psychology, Health & MedicineDocument12 pagesPsychology, Health & MedicineArturo MelgarNo ratings yet
- Recognition of Child Abuse for the Mandated Reporter 4eFrom EverandRecognition of Child Abuse for the Mandated Reporter 4eNo ratings yet
- Sexual Abuse and Sexual Risk Behavior, Beyond The ImpactDocument11 pagesSexual Abuse and Sexual Risk Behavior, Beyond The Impacthussi.musajiNo ratings yet
- Early Childhood Trauma Treatments: Considerations for CliniciansDocument14 pagesEarly Childhood Trauma Treatments: Considerations for CliniciansClaudia Irma Portilla CamposNo ratings yet
- Association Between Childhood Trauma, Parental Bonding and Antisocial A Machine Learning ApproachDocument5 pagesAssociation Between Childhood Trauma, Parental Bonding and Antisocial A Machine Learning ApproachTara aNo ratings yet
- Cumulative Effects of Childhood Traumas - Polytraumatization, Dissociation, and Schizophrenia PDFDocument10 pagesCumulative Effects of Childhood Traumas - Polytraumatization, Dissociation, and Schizophrenia PDFguswendyw_201473766No ratings yet
- Dissertation Mental Health StigmaDocument8 pagesDissertation Mental Health StigmaNeedSomeoneWriteMyPaperIndianapolis100% (1)
- Long-Term Consequences of Childhood Sexual Abuse by Gender of VictimDocument9 pagesLong-Term Consequences of Childhood Sexual Abuse by Gender of VictimMalyasree BasuNo ratings yet
- Mond 2010klkoojljljlDocument20 pagesMond 2010klkoojljljlverghese17No ratings yet
- Running Head: MENTAL DISORDERS 1Document12 pagesRunning Head: MENTAL DISORDERS 1api-532509198No ratings yet
- Child NF Paper 6 - 12 - 2020 FFDocument29 pagesChild NF Paper 6 - 12 - 2020 FFabelim01No ratings yet
- Adverse Effects of Child Abuse on DevelopmentDocument5 pagesAdverse Effects of Child Abuse on DevelopmentJerry EspinosaNo ratings yet
- Kaminski Clausse (2017)Document24 pagesKaminski Clausse (2017)Nuria Moreno RománNo ratings yet
- 1 s2.0 S0145213410002243 MainDocument14 pages1 s2.0 S0145213410002243 Mainathaya malika rahmanNo ratings yet
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsFrom EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNo ratings yet
- Best Practice & Research Clinical Obstetrics and Gynaecology article discusses abortion and subsequent life outcomesDocument12 pagesBest Practice & Research Clinical Obstetrics and Gynaecology article discusses abortion and subsequent life outcomesCristina ToaderNo ratings yet
- Álvarez Et Al (2011) ChildabuseDocument6 pagesÁlvarez Et Al (2011) ChildabuseAra Moreno EscaladaNo ratings yet
- Summary PaperDocument8 pagesSummary PaperLogan CarterNo ratings yet
- Child Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsFrom EverandChild Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsNo ratings yet
- Physicians' Use of Inclusive Language During Teen VisitsDocument9 pagesPhysicians' Use of Inclusive Language During Teen VisitsTherese Berina-MallenNo ratings yet
- Dating Violence Perpetration and Victimization Among U.S. Adolescents: Prevalence, Patterns, and Associations With Health Complaints and Substance UseDocument8 pagesDating Violence Perpetration and Victimization Among U.S. Adolescents: Prevalence, Patterns, and Associations With Health Complaints and Substance UseAlba EneaNo ratings yet
- The Impact of Living With Klinefelter Syndrome: A Qualitative Exploration of Adolescents and AdultsDocument10 pagesThe Impact of Living With Klinefelter Syndrome: A Qualitative Exploration of Adolescents and AdultsصادقNo ratings yet
- Parent and Child Knowledge and Attitudes Toward Mental Illness: A Pilot StudyDocument11 pagesParent and Child Knowledge and Attitudes Toward Mental Illness: A Pilot StudySteluta AureliaNo ratings yet
- Gender Perspective in Dual DiagnosisDocument4 pagesGender Perspective in Dual DiagnosisBalmaNo ratings yet
- Human Trafficking Health Research Progress and Future DirectionsDocument5 pagesHuman Trafficking Health Research Progress and Future DirectionsIan AdarveNo ratings yet
- Patrick Esposito MaltreatmentDocument5 pagesPatrick Esposito Maltreatmentapi-313736865No ratings yet
- Children with Incarcerated Mothers: Separation, Loss, and ReunificationFrom EverandChildren with Incarcerated Mothers: Separation, Loss, and ReunificationJulie Poehlmann-TynanNo ratings yet
- Adverse Childhood Experiences and Coping Strategies: Identifying Pathways To Resiliency in AdulthoodDocument17 pagesAdverse Childhood Experiences and Coping Strategies: Identifying Pathways To Resiliency in AdulthoodAndreea PalNo ratings yet
- Intimate Partner Violence: A Resource for Professionals Working With Children and FamiliesFrom EverandIntimate Partner Violence: A Resource for Professionals Working With Children and FamiliesNo ratings yet
- Terapy YouthDocument6 pagesTerapy YouthHassaelNo ratings yet
- A Comparison of Sexual Minority Youth Who Attend Religiously Affiliated Schools and Their Nonreligious-School-Attending CounterpartsDocument20 pagesA Comparison of Sexual Minority Youth Who Attend Religiously Affiliated Schools and Their Nonreligious-School-Attending CounterpartsVon BravanteNo ratings yet
- The Context of Condom Use Among Young Adults in The Philippines: Implications For HIV PreventionDocument23 pagesThe Context of Condom Use Among Young Adults in The Philippines: Implications For HIV PreventionJessieRealistaNo ratings yet
- Child Abuse & Neglect: Robyn Brunton, Rachel DryerDocument16 pagesChild Abuse & Neglect: Robyn Brunton, Rachel DryerDiego ZambranoNo ratings yet
- Blasco 2018Document18 pagesBlasco 2018febrianeNo ratings yet
- Puberty Suppression Medicine or MalpracticeDocument35 pagesPuberty Suppression Medicine or Malpracticebashomatsuo50% (2)
- Guide to Intellectual Disabilities: A Clinical HandbookFrom EverandGuide to Intellectual Disabilities: A Clinical HandbookJulie P. GentileNo ratings yet
- The Education, Wellbeing and Identity of Children With Migrant or Refugee BackgroundsDocument72 pagesThe Education, Wellbeing and Identity of Children With Migrant or Refugee BackgroundsDonald Cabrera AstudilloNo ratings yet
- Strategic Inhibitio of Distractors With Visual Working Memory Contents After Involuntary Attention CaptureDocument9 pagesStrategic Inhibitio of Distractors With Visual Working Memory Contents After Involuntary Attention CaptureDonald Cabrera AstudilloNo ratings yet
- Measurement Issues - Measurement of Posttraumatic Stress Disorder in Children and Young People - Lessons From Research and PracticeDocument12 pagesMeasurement Issues - Measurement of Posttraumatic Stress Disorder in Children and Young People - Lessons From Research and PracticeDonald Cabrera AstudilloNo ratings yet
- Psychiatric Comorbidity in Childhood and Adolescence HeadacheDocument8 pagesPsychiatric Comorbidity in Childhood and Adolescence HeadacheDonald Cabrera AstudilloNo ratings yet
- PTSD in Children and Adolescents - Toward An Empirically Based AlgorithmDocument13 pagesPTSD in Children and Adolescents - Toward An Empirically Based AlgorithmDonald Cabrera AstudilloNo ratings yet
- Do Gender and Age Moderate The Symptom Structure of PTSD - Findings From A National Clinical Sample of Children and AdolescentsDocument9 pagesDo Gender and Age Moderate The Symptom Structure of PTSD - Findings From A National Clinical Sample of Children and AdolescentsDonald Cabrera AstudilloNo ratings yet
- Predicting PTSD From The Child Behavior Checklist - Data From A Field Study With Children and Adolescents in Foster CareDocument6 pagesPredicting PTSD From The Child Behavior Checklist - Data From A Field Study With Children and Adolescents in Foster CareDonald Cabrera AstudilloNo ratings yet
- Social, Psychological, and Psychiatric Interventions Following Terrorist Attacks - Recommendations For Practice and ResearchDocument13 pagesSocial, Psychological, and Psychiatric Interventions Following Terrorist Attacks - Recommendations For Practice and ResearchDonald Cabrera AstudilloNo ratings yet
- Relating Pattern Deviancy Aversion To Stigma and PrejudiceDocument11 pagesRelating Pattern Deviancy Aversion To Stigma and PrejudiceDonald Cabrera AstudilloNo ratings yet
- The Child Posttraumatic Stress Disorder Checklist in A Sample of South African YouthDocument7 pagesThe Child Posttraumatic Stress Disorder Checklist in A Sample of South African YouthDonald Cabrera AstudilloNo ratings yet
- Annual Research Review - Attachment Disorders in Early Childhood - Clinical Presentation, Causes, Correlates, and TreatmentDocument16 pagesAnnual Research Review - Attachment Disorders in Early Childhood - Clinical Presentation, Causes, Correlates, and TreatmentDonald Cabrera Astudillo0% (1)
- Validation of The UCLA Child Post Traumatic Stress Disorder-Reaction Index in ZambiaDocument13 pagesValidation of The UCLA Child Post Traumatic Stress Disorder-Reaction Index in ZambiaDonald Cabrera AstudilloNo ratings yet
- From Soldiers To Children - Developmental Sciences Transform The Construct of Posttraumatic Stress DisorderDocument16 pagesFrom Soldiers To Children - Developmental Sciences Transform The Construct of Posttraumatic Stress DisorderDonald Cabrera AstudilloNo ratings yet
- Factors Affecting The Diagnosis and Prediction of PTSD PDFDocument8 pagesFactors Affecting The Diagnosis and Prediction of PTSD PDFAGRANo ratings yet
- Validity Issues in Transcultural EpidemiologyDocument4 pagesValidity Issues in Transcultural EpidemiologyDonald Cabrera AstudilloNo ratings yet
- PTSD Symptoms in Young Children Exposed To Intimate Partner Violence in Four Ethno-Racial GroupsDocument11 pagesPTSD Symptoms in Young Children Exposed To Intimate Partner Violence in Four Ethno-Racial GroupsDonald Cabrera AstudilloNo ratings yet
- Trauma in Early Childhood: A Neglected PopulationDocument20 pagesTrauma in Early Childhood: A Neglected PopulationFrancisca AldunateNo ratings yet
- Annual Research Review Enduring Neurobiological Effects of Childhood Abuse and NeglectDocument26 pagesAnnual Research Review Enduring Neurobiological Effects of Childhood Abuse and NeglectDonald Cabrera AstudilloNo ratings yet
- PTSDDocument12 pagesPTSDAGRANo ratings yet
- The Phylogenetic Roots of Human Lethal ViolenceDocument10 pagesThe Phylogenetic Roots of Human Lethal ViolenceDonald Cabrera AstudilloNo ratings yet
- The Phylogenetic Roots of Human Lethal ViolenceDocument10 pagesThe Phylogenetic Roots of Human Lethal ViolenceDonald Cabrera AstudilloNo ratings yet
- The Neurobiology of Aggression and ViolenceDocument27 pagesThe Neurobiology of Aggression and ViolenceDonald Cabrera AstudilloNo ratings yet
- The Neurobiology of Disryptive Behavior DisorderDocument2 pagesThe Neurobiology of Disryptive Behavior DisorderDonald Cabrera AstudilloNo ratings yet
- The Neurobiology of Disryptive Behavior DisorderDocument2 pagesThe Neurobiology of Disryptive Behavior DisorderDonald Cabrera AstudilloNo ratings yet
- The Nature of Human AggressionDocument7 pagesThe Nature of Human AggressionDonald Cabrera AstudilloNo ratings yet
- Reduced Brain Activation in Violent Adolescents During Response InhibitionDocument7 pagesReduced Brain Activation in Violent Adolescents During Response InhibitionDonald Cabrera AstudilloNo ratings yet
- The Nature of Human AggressionDocument7 pagesThe Nature of Human AggressionDonald Cabrera AstudilloNo ratings yet
- Neurobiology of Attachment To An Abusive Caregiver - Short-Term Benefits and Long-Term CostsDocument9 pagesNeurobiology of Attachment To An Abusive Caregiver - Short-Term Benefits and Long-Term CostsDonald Cabrera AstudilloNo ratings yet
- The Concept of Violent Suicide, Its Underlying Trait and Neurobiology - A Critical PerspectiveDocument9 pagesThe Concept of Violent Suicide, Its Underlying Trait and Neurobiology - A Critical PerspectiveDonald Cabrera AstudilloNo ratings yet
- The Neurobiology of Aggression and ViolenceDocument27 pagesThe Neurobiology of Aggression and ViolenceDonald Cabrera AstudilloNo ratings yet
- NewyorkDocument8 pagesNewyorkapi-280868990No ratings yet
- Different Types of CrimeDocument2 pagesDifferent Types of CrimeKatia AssisNo ratings yet
- Social Issues in inDocument4 pagesSocial Issues in inaanand210% (1)
- El Salvador ms-13Document3 pagesEl Salvador ms-13api-255702164No ratings yet
- Total Prospectus July 2019 - 1562663614 PDFDocument119 pagesTotal Prospectus July 2019 - 1562663614 PDFKnowledge GuruNo ratings yet
- Orientation On Gender SensitivityDocument67 pagesOrientation On Gender SensitivityCalapati, Jhon Rovic R.No ratings yet
- Goodluck Jonathan: A President in Search of A LegacyDocument3 pagesGoodluck Jonathan: A President in Search of A LegacyEwoigbokhan Otaigbe ItuaNo ratings yet
- El Abuso Sexual Basado en Imágenes DeepfakeDocument9 pagesEl Abuso Sexual Basado en Imágenes DeepfakeRoberto Lemaitre PicadoNo ratings yet
- Geriatric CareDocument24 pagesGeriatric CareDr. Jayesh Patidar0% (1)
- Applying Space Transition Theory To Cyber Crime A Theoretical Analysis of Revenge Pornography in The 21st CenturyDocument7 pagesApplying Space Transition Theory To Cyber Crime A Theoretical Analysis of Revenge Pornography in The 21st CenturyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Tyler Green 1Document5 pagesTyler Green 1Tyler GreenNo ratings yet
- OwenDocument10 pagesOwenJuan SanchezNo ratings yet
- Mens Behaviour Change Program BrochureDocument2 pagesMens Behaviour Change Program BrochureayzlimNo ratings yet
- Palomarez 1st Amended Verified PetitionDocument13 pagesPalomarez 1st Amended Verified PetitionMaria PeñaNo ratings yet
- Secure Base ChecklistDocument15 pagesSecure Base ChecklistSaul PsiqNo ratings yet
- Agreement To Mediate - CCR FormDocument1 pageAgreement To Mediate - CCR FormEzekiel KobinaNo ratings yet
- PPTDocument11 pagesPPTAaroh Srivastava100% (1)
- Research ProposalDocument35 pagesResearch ProposalMulugeta Bariso100% (3)
- LGBTQ+ students face discrimination in Philippine schoolsDocument2 pagesLGBTQ+ students face discrimination in Philippine schoolsJames AmponganNo ratings yet
- Crimes Committed by Public Officers (203-245) : Only Just SomeDocument13 pagesCrimes Committed by Public Officers (203-245) : Only Just SomeChristopher PjunatasNo ratings yet
- Domestic Violence Prevention and Protection Act 2012Document8 pagesDomestic Violence Prevention and Protection Act 2012Xahid HasanNo ratings yet
- Models of Different Types of Editorials on Ending School BullyingDocument1 pageModels of Different Types of Editorials on Ending School BullyingJoshkorro GeronimoNo ratings yet
- Persepolis EssayDocument4 pagesPersepolis Essayapi-302460347No ratings yet
- Evidence of Marc Randazza's Associate Ari Bass Aka Michael Whiteacre Stalking Alexandra Mayers - Randazza NewsDocument3 pagesEvidence of Marc Randazza's Associate Ari Bass Aka Michael Whiteacre Stalking Alexandra Mayers - Randazza NewsCrystal CoxNo ratings yet
- Human Trafficking YouthDocument59 pagesHuman Trafficking YouthJanetGraceDalisayFabreroNo ratings yet
- The Singing Challenge Britain's Got Talent Hopeful Student's WorksheetDocument4 pagesThe Singing Challenge Britain's Got Talent Hopeful Student's WorksheetAngel Angeleri-priftis.No ratings yet
- CRDP African American Report PDFDocument379 pagesCRDP African American Report PDFiggybauNo ratings yet
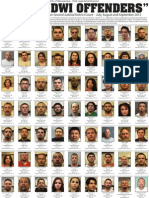
- Guilty DWI Offenders - August-September 2012Document2 pagesGuilty DWI Offenders - August-September 2012Albuquerque JournalNo ratings yet
- The Lorax Tasia RasmussenDocument5 pagesThe Lorax Tasia Rasmussenapi-252001729No ratings yet
- CPN-CSPC Protocol 26nov2014Document136 pagesCPN-CSPC Protocol 26nov2014John J. MacasioNo ratings yet