You might also like
- CK 12 Earth Science Concepts For Middle School B v14 Ha5 s1Document1,194 pagesCK 12 Earth Science Concepts For Middle School B v14 Ha5 s1JTKirk61100% (1)
- Knave 2 Kickstarter Draft 6Document43 pagesKnave 2 Kickstarter Draft 6Máté Gergely BaloghNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The ART of Reading Smoke in 40 CharactersDocument36 pagesThe ART of Reading Smoke in 40 CharactersMarco London100% (1)
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Document13 pagesSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanNo ratings yet
- Practice Exam 2Document22 pagesPractice Exam 2Sealtiel1020100% (1)
- Nosocomial Infection?Document4 pagesNosocomial Infection?Sara ANo ratings yet
- Types of Seizure & Status Epilepticus: Prepared By: Ivy Joy A. Benitez, BSN 4-ADocument28 pagesTypes of Seizure & Status Epilepticus: Prepared By: Ivy Joy A. Benitez, BSN 4-AyviyojNo ratings yet
- Approach To An Unconscious Patient-OyeyemiDocument41 pagesApproach To An Unconscious Patient-OyeyemiOyeyemi AdeyanjuNo ratings yet
- Peds QuestionsDocument8 pagesPeds QuestionsKiranNo ratings yet
- Care of The Hospitalized ChildDocument60 pagesCare of The Hospitalized ChildJSeasharkNo ratings yet
- Ivo Andric Woman From SarajevoDocument253 pagesIvo Andric Woman From SarajevoDanijel JurićNo ratings yet
- NasoGastric Tube FeedingDocument3 pagesNasoGastric Tube FeedingSwati SharmaNo ratings yet
- Guiilan Barre SyndromeDocument19 pagesGuiilan Barre SyndromeDhayaneeDruAinsleyIINo ratings yet
- Newborn CareDocument49 pagesNewborn CareJohn Mark PocsidioNo ratings yet
- Ydt 2010-2022 Ösym Çikmiş SorularDocument323 pagesYdt 2010-2022 Ösym Çikmiş SorularNobodyNo ratings yet
- Seminar ON: Communicable DiseasesDocument159 pagesSeminar ON: Communicable DiseasesvishnuNo ratings yet
- JBI Scoping Review Manual 2020 p1-3 PDFDocument4 pagesJBI Scoping Review Manual 2020 p1-3 PDFkusrini_kadarNo ratings yet
- Quality AssuranceDocument74 pagesQuality Assurancepreeti1998767% (3)
- Administration of MedicationDocument18 pagesAdministration of MedicationThilaga RamNo ratings yet
- Pediatric Liver Transplant AssessmentDocument30 pagesPediatric Liver Transplant AssessmentMadhu Sinha100% (1)
- Pediatric Nursing BookDocument371 pagesPediatric Nursing Bookmathio medhatNo ratings yet
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Answer Key To English Advanced Vocabulary and Structure PracticeDocument6 pagesAnswer Key To English Advanced Vocabulary and Structure PracticeMinhHD50% (2)
- Zero Energy Buildings and Sustainable Development Implications - A ReviewDocument10 pagesZero Energy Buildings and Sustainable Development Implications - A ReviewJoao MinhoNo ratings yet
- Types of Skin Traction PresentationDocument16 pagesTypes of Skin Traction PresentationZerjohn Seniorom100% (1)
- Case Report "Febrile Seizures": Betsheba E. S. 123307018Document37 pagesCase Report "Febrile Seizures": Betsheba E. S. 123307018AmandaRizkaNo ratings yet
- Chest Physiotherapy - Postural DrainageDocument2 pagesChest Physiotherapy - Postural DrainageMicah MagallanoNo ratings yet
- Bronchodilators Guide for Asthma and COPDDocument5 pagesBronchodilators Guide for Asthma and COPDdeepika kushwahNo ratings yet
- Oxygen Therapy and Oxygen Delivery (Pediatric) - CEDocument8 pagesOxygen Therapy and Oxygen Delivery (Pediatric) - CEViviana AltamiranoNo ratings yet
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)
- HumidificationDocument7 pagesHumidificationSiva ShanmugamNo ratings yet
- Infant Radiant WarmerDocument7 pagesInfant Radiant WarmerManish MandaviyaNo ratings yet
- Class II Neurotic DisordersDocument37 pagesClass II Neurotic DisordersNarayan K Ghorapde100% (1)
- Assessment of Beonate - FN - IIIDocument79 pagesAssessment of Beonate - FN - IIIashamartinaNo ratings yet
- Nursing Care PneumoniaDocument26 pagesNursing Care PneumoniaIsaac Kipkemoi100% (1)
- Nurses' competence in examining sexually assaulted persons: A comparison of Canada and NigeriaDocument25 pagesNurses' competence in examining sexually assaulted persons: A comparison of Canada and NigeriaWasiu AfoloabiNo ratings yet
- Assessing the Normal NewbornDocument97 pagesAssessing the Normal NewbornettevyviNo ratings yet
- Tetanus: HistoryDocument15 pagesTetanus: HistorydanielleNo ratings yet
- CONTROLLINGpptDocument40 pagesCONTROLLINGpptDarren Flores100% (1)
- StrokeDocument6 pagesStrokeRaulLopezJaimeNo ratings yet
- CPMS Nursing Procedure for IV InjectionDocument5 pagesCPMS Nursing Procedure for IV InjectionAmy LalringhluaniNo ratings yet
- Meningitis PPT 2.0Document15 pagesMeningitis PPT 2.0Francis Adrian100% (1)
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDocument12 pagesMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RNo ratings yet
- DehydrationDocument19 pagesDehydrationIlyes FerenczNo ratings yet
- Shoulder Pain Case- Secondary Adhesive CapsulitisDocument44 pagesShoulder Pain Case- Secondary Adhesive CapsulitisSonali JoshiNo ratings yet
- Pediatric NotesDocument4 pagesPediatric NotesJincy PrinceNo ratings yet
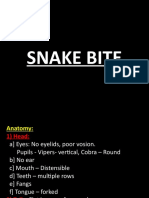
- Snake BiteDocument61 pagesSnake Biteniraj_sdNo ratings yet
- Control Bleeding with Direct PressureDocument14 pagesControl Bleeding with Direct PressureRhomizal MazaliNo ratings yet
- Hirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument6 pagesHirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- Birth asphyxia causes and neonatal resuscitationDocument20 pagesBirth asphyxia causes and neonatal resuscitationinne_fNo ratings yet
- Application of Health Belief Model in NursingDocument5 pagesApplication of Health Belief Model in NursingWilson Machado0% (1)
- Respiratory Disorder Note BSC 3rd YearDocument41 pagesRespiratory Disorder Note BSC 3rd YearNancyNo ratings yet
- Nursing Education Records & ReportsDocument18 pagesNursing Education Records & ReportsmagieNo ratings yet
- SUBDocument18 pagesSUBArun KumarNo ratings yet
- Nursing Care Plans For Diabetes MellitusDocument12 pagesNursing Care Plans For Diabetes MellitusPuteri AzmanNo ratings yet
- Pain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalDocument50 pagesPain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalPrathiba PrassaddNo ratings yet
- ARTICLESDocument20 pagesARTICLESJenish Panchal100% (1)
- RHEUMATIC FEVER: A MULTISYSTEM DISEASEDocument24 pagesRHEUMATIC FEVER: A MULTISYSTEM DISEASErameshbmcNo ratings yet
- Asthma Management and Prevention in ChildrenDocument57 pagesAsthma Management and Prevention in ChildrenSundararajaperumal AnandhakrishnanNo ratings yet
- Assessing Newborns EffectivelyDocument35 pagesAssessing Newborns EffectivelyBaldwin Hamzcorp Hamoonga100% (1)
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 pagesTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaNo ratings yet
- HydronephrosisDocument2 pagesHydronephrosisGanis RyNo ratings yet
- Kenya ARV Guidelines 2018Document230 pagesKenya ARV Guidelines 2018Felix Wafula MusibiNo ratings yet
- Case Presentation On Tennis Elbow: Sudipta BhowmickDocument16 pagesCase Presentation On Tennis Elbow: Sudipta BhowmickNeha BhasinNo ratings yet
- Hepatitis in ChildrenDocument2 pagesHepatitis in ChildrenShilpi SinghNo ratings yet
- Myelography Procedure and Indications ExplainedDocument12 pagesMyelography Procedure and Indications ExplainedDiana CharaNo ratings yet
- Lens Related GlaucomaDocument19 pagesLens Related GlaucomaUsama ButtNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Coaching Dan CommunicationDocument10 pagesCoaching Dan Communicationkusrini_kadarNo ratings yet
- Types of Printed Educational Material For Pregnancy in IndonesiaDocument1 pageTypes of Printed Educational Material For Pregnancy in Indonesiakusrini_kadarNo ratings yet
- Patient Education Materials Assessment Tool For Printable Materials (PEMAT-P)Document4 pagesPatient Education Materials Assessment Tool For Printable Materials (PEMAT-P)kusrini_kadarNo ratings yet
- Suitability Assessment of Materials (SAM) : at Desirable Reader Behavior Rather Than Nonbehavior FactsDocument7 pagesSuitability Assessment of Materials (SAM) : at Desirable Reader Behavior Rather Than Nonbehavior Factskusrini_kadarNo ratings yet
- Health Education Materials Assessment ToolDocument6 pagesHealth Education Materials Assessment Toolkusrini_kadarNo ratings yet
- Oral Presentation Schedule - 20190715Document25 pagesOral Presentation Schedule - 20190715kusrini_kadarNo ratings yet
- Merged 20200416 230127 PDFDocument16 pagesMerged 20200416 230127 PDFkusrini_kadarNo ratings yet
- Curriculum Vitae Summary for Nursing LecturerDocument3 pagesCurriculum Vitae Summary for Nursing Lecturerkusrini_kadarNo ratings yet
- Ageing in Indonesia - Health Status and Challenges For The FutureDocument10 pagesAgeing in Indonesia - Health Status and Challenges For The Futurekusrini_kadarNo ratings yet
- 028 - National Protect SealDocument4 pages028 - National Protect SealMohammed Sayeeduddin100% (1)
- IR Rework Setup and Profile SettingsDocument18 pagesIR Rework Setup and Profile SettingsZach LeedyNo ratings yet
- Concrete Pavement - Group 8Document8 pagesConcrete Pavement - Group 8Bryan YuNo ratings yet
- Voices 4 End-of-Term Exam Standard Units 7-9: VocabularyDocument10 pagesVoices 4 End-of-Term Exam Standard Units 7-9: VocabularyAnaNo ratings yet
- Test Bank For Corporate Financial Accounting 14th Edition by Warren ISBN 130565353X 9781305653535Document36 pagesTest Bank For Corporate Financial Accounting 14th Edition by Warren ISBN 130565353X 9781305653535isaiahpiercetwrxokmsdp100% (24)
- Growing GarlicDocument2 pagesGrowing GarlicCarlos L Diaz GonzalezNo ratings yet
- H. Spencer Lewis, Astrology and Tarot (1907)Document5 pagesH. Spencer Lewis, Astrology and Tarot (1907)Alois HaasNo ratings yet
- IMCORRDocument247 pagesIMCORRSebastián Esteban Cisternas GuzmánNo ratings yet
- The Indian BorderlandDocument463 pagesThe Indian BorderlandBilal AfridiNo ratings yet
- Testconsult TDR2 Pile Integrity Tester WV1.0 PDFDocument2 pagesTestconsult TDR2 Pile Integrity Tester WV1.0 PDFTayfun ünverNo ratings yet
- Vol37 3Document522 pagesVol37 3Nguyen HongNo ratings yet
- Week #3 - What Makes Swing?Document1 pageWeek #3 - What Makes Swing?Gareth James ParryNo ratings yet
- ConvalescenceDocument18 pagesConvalescenceVictorNo ratings yet
- Air Quality HandbookDocument249 pagesAir Quality HandbookMarc Jyron Sayat ManacapNo ratings yet
- Is 7861-1976 Part 1 Code of Practice For Extreme Weather Concreting Part 1 Recommended Practice FDocument23 pagesIs 7861-1976 Part 1 Code of Practice For Extreme Weather Concreting Part 1 Recommended Practice FAnmil Singh100% (1)
- Plants Adapt to Environmental Factors Through Morphological, Anatomical and Physiological ChangesDocument25 pagesPlants Adapt to Environmental Factors Through Morphological, Anatomical and Physiological Changessrk2005No ratings yet
- M GV4 Piccolo-Install 20170428Document24 pagesM GV4 Piccolo-Install 20170428Anonymous M0OEZEKoGiNo ratings yet
- Ecohydrology As An Important Concept and Tool inDocument3 pagesEcohydrology As An Important Concept and Tool inCésar SuazaNo ratings yet
- 2.1 Cows ..2 2.2 Pits .4 2.3 Chaos .5Document23 pages2.1 Cows ..2 2.2 Pits .4 2.3 Chaos .5AntonNo ratings yet
- Conditionals: Conditional SentencesDocument3 pagesConditionals: Conditional SentencesDJ Johan-MNo ratings yet
- Semester (1.5y) : Sarhad Intitue of Resarch and Education Lakki MarwatDocument6 pagesSemester (1.5y) : Sarhad Intitue of Resarch and Education Lakki MarwatSadam IrshadNo ratings yet
- 40 câu hỏi tiếng AnhDocument5 pages40 câu hỏi tiếng AnhLe ThyNo ratings yet