You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Power Point Pulse OximetryDocument11 pagesPower Point Pulse Oximetryanon_47299004No ratings yet
- Pathological Gait Patterns in Coxa Retrotorta in Pediatric Population-Supplementary Examination For Preoperative Planning?Document2 pagesPathological Gait Patterns in Coxa Retrotorta in Pediatric Population-Supplementary Examination For Preoperative Planning?Gabriela Istrati-StanciugelNo ratings yet
- Integrated Hospital Management SystemDocument12 pagesIntegrated Hospital Management SystemPayal ThakkerNo ratings yet
- Musculoskeletal News PDFDocument4 pagesMusculoskeletal News PDFΑΛΕΞΗΣ ΙΩΑΝΝΟΥNo ratings yet
- Review Article: Occlusal Schemes For Complete Dentures - A Review ArticleDocument6 pagesReview Article: Occlusal Schemes For Complete Dentures - A Review ArticleoktikikiNo ratings yet
- Dental FluorosisDocument8 pagesDental Fluorosiskuantumonline100% (1)
- Documents Emerge Proving DR Andrew Wakefield Innocent BMJ and Brian Deer Caught Misrepresenting The FactsDocument5 pagesDocuments Emerge Proving DR Andrew Wakefield Innocent BMJ and Brian Deer Caught Misrepresenting The Factsjamie_clark_2100% (1)
- Lupus NeonatalDocument2 pagesLupus NeonatalFer45No ratings yet
- History of the stethoscopeDocument2 pagesHistory of the stethoscopepswaminathan100% (1)
- Down Syndrome: An Overview: March 2016Document7 pagesDown Syndrome: An Overview: March 2016Hartotok VipnetNo ratings yet
- Jurnal AntibiotikDocument5 pagesJurnal AntibiotikSela PutrianaNo ratings yet
- Wrist WikiRadDocument34 pagesWrist WikiRadGriggrogGingerNo ratings yet
- Diagnostic Approach To Fetal MicrocephalyDocument9 pagesDiagnostic Approach To Fetal MicrocephalyAlif BareizyNo ratings yet
- Toxic Ingestions Pediatric EmergencyDocument24 pagesToxic Ingestions Pediatric EmergencyXimenaEspinaNo ratings yet
- Brodsky 2004Document14 pagesBrodsky 2004Ervan SuryaNo ratings yet
- ChronOS InjecDocument24 pagesChronOS Injecmolecule112No ratings yet
- Jurnal Terapi CA ColonDocument4 pagesJurnal Terapi CA ColonyopiNo ratings yet
- Pedo 1 PDFDocument9 pagesPedo 1 PDFaccangNo ratings yet
- Double Outlet Right VentricleDocument5 pagesDouble Outlet Right VentricleB-win IrawanNo ratings yet
- Transform NIfTI volume orientation with reslice_niiDocument31 pagesTransform NIfTI volume orientation with reslice_niiMiguel Moreno EstévezNo ratings yet
- Patient Evaluation and Wound Assessment: Key Practice PointsDocument6 pagesPatient Evaluation and Wound Assessment: Key Practice PointsFofiuNo ratings yet
- 6th ANU 2022 Final FLYERDocument2 pages6th ANU 2022 Final FLYERAgung Arga LabuanNo ratings yet
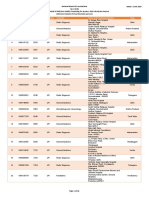
- Allotment Details of DNB Final Round Counseling for January 2019Document48 pagesAllotment Details of DNB Final Round Counseling for January 2019Raghul KrishnasamyNo ratings yet
- Assessing Vertebral Fractures Using Semiquantitative TechniqueDocument12 pagesAssessing Vertebral Fractures Using Semiquantitative TechniqueDenise CortinovisNo ratings yet
- Ltyg Quick Start GuideDocument22 pagesLtyg Quick Start Guidemarkus_naslundNo ratings yet
- 2005 AFA InglesDocument5 pages2005 AFA InglesAgatha Nascimento Dos SantosNo ratings yet
- Catalogo RmoDocument301 pagesCatalogo RmochachocaraNo ratings yet
- 5 6275917323719147718 PDFDocument771 pages5 6275917323719147718 PDFKousik AmancharlaNo ratings yet
- Gastric Emptying and Hepatitis MortalityDocument285 pagesGastric Emptying and Hepatitis Mortalityjielani100% (1)
- WFA Competency LevelsDocument5 pagesWFA Competency LevelsTroy Lyons DunowNo ratings yet