You might also like
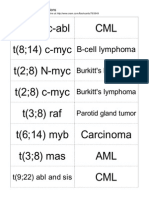
- Translocations Small00center10 765849Document5 pagesTranslocations Small00center10 765849dger11No ratings yet
- Translocations Small00center10 765849Document5 pagesTranslocations Small00center10 765849dger11No ratings yet
- Klyosov 1Document31 pagesKlyosov 1dger11No ratings yet
- Squamous Cell Carcinoma of The LungDocument2 pagesSquamous Cell Carcinoma of The Lungdger11No ratings yet
- Luntz Wexner AnalysisDocument17 pagesLuntz Wexner Analysisdger11No ratings yet
- Congenital Cytomegalovirus InfectionDocument5 pagesCongenital Cytomegalovirus Infectiondger11No ratings yet
- Translocations Small00center10 765849Document5 pagesTranslocations Small00center10 765849dger11No ratings yet
- Vertically Transmitted InfectionDocument6 pagesVertically Transmitted Infectiondger11No ratings yet
- Medullary Thyroid CancerDocument5 pagesMedullary Thyroid Cancerdger11No ratings yet
- Allergic Bronchopulmonary AspergillosisDocument6 pagesAllergic Bronchopulmonary Aspergillosisdger11No ratings yet
- Deci Dual IzationDocument2 pagesDeci Dual Izationdger11No ratings yet
- Pneumocystis Pneumonia Diagnosis and TreatmentDocument5 pagesPneumocystis Pneumonia Diagnosis and Treatmentdger11No ratings yet
- Atrophic VaginitisDocument3 pagesAtrophic Vaginitisdger11No ratings yet
- The Flyting of Dunbar and KennedyDocument25 pagesThe Flyting of Dunbar and KennedyCholo MercadoNo ratings yet
- Renal Cell CarcinomaDocument15 pagesRenal Cell Carcinomadger11No ratings yet
- Cancer SyndromeDocument6 pagesCancer Syndromedger11No ratings yet
- Congenital Cytomegalovirus InfectionDocument5 pagesCongenital Cytomegalovirus Infectiondger11No ratings yet
- Nodular Fasciitis: Etiology and Clinical CourseDocument3 pagesNodular Fasciitis: Etiology and Clinical Coursedger11No ratings yet
- Vertically Transmitted InfectionDocument6 pagesVertically Transmitted Infectiondger11No ratings yet
- Squamous Cell Carcinoma of The LungDocument2 pagesSquamous Cell Carcinoma of The Lungdger11No ratings yet
- Medullary Thyroid CancerDocument5 pagesMedullary Thyroid Cancerdger11No ratings yet
- Anglo SaxonDocument4 pagesAnglo Saxondger11No ratings yet
- Viking00barr BWDocument154 pagesViking00barr BWdger11No ratings yet
- Allergic Bronchopulmonary AspergillosisDocument6 pagesAllergic Bronchopulmonary Aspergillosisdger11No ratings yet
- The Flyting of Dunbar and KennedyDocument25 pagesThe Flyting of Dunbar and KennedyCholo MercadoNo ratings yet
- Outlines in PathologyDocument200 pagesOutlines in PathologyLisztomaniaNo ratings yet
- Vuk Stefanovic Karadzic: Srpski Rjecnik (1898)Document935 pagesVuk Stefanovic Karadzic: Srpski Rjecnik (1898)krca100% (2)
- Calender of The Close RollsDocument938 pagesCalender of The Close Rollsdger11No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Its A Simple Test Cervical Cancer Screening UrduDocument1 pageIts A Simple Test Cervical Cancer Screening UrduIqbal BaryarNo ratings yet
- Terapi Lesi Pra-Kanker Leher Rahim (Krioterapi)Document31 pagesTerapi Lesi Pra-Kanker Leher Rahim (Krioterapi)yulia gustiNo ratings yet
- 1-General Table For Screening - LockedDocument34 pages1-General Table For Screening - LockedChristian Yzaguirre AbantoNo ratings yet
- Ovarian Cancer TypesDocument60 pagesOvarian Cancer TypesLeslie Ann Pablo MarantanNo ratings yet
- Survival Outcomes For Different Subtypes of Epithelial Ovarian CancerDocument7 pagesSurvival Outcomes For Different Subtypes of Epithelial Ovarian CancerasclepiuspdfsNo ratings yet
- Pathology of The Female Genital Tract Course OutlineDocument2 pagesPathology of The Female Genital Tract Course OutlineDanica BiteraNo ratings yet
- Lesi Prakanker & Tumor Ginekologi (Versi 2003)Document71 pagesLesi Prakanker & Tumor Ginekologi (Versi 2003)Satwika EkanandaNo ratings yet
- Artikel Trias Mei Purnama AnggrainiDocument10 pagesArtikel Trias Mei Purnama AnggrainiRenandaNo ratings yet
- 2014 AsccpDocument62 pages2014 AsccpGia DuyNo ratings yet
- CCSP GuidelinesDocument42 pagesCCSP GuidelinesAzhagendranNo ratings yet
- Management of Abnormal Pap Smears PresentationDocument17 pagesManagement of Abnormal Pap Smears Presentationapi-210786702100% (1)
- TAMIZACION CANCER DE CUELLO UTERINO EN COLOMBIADocument53 pagesTAMIZACION CANCER DE CUELLO UTERINO EN COLOMBIALUIS FERNANDO PLAZAS MUNOZNo ratings yet
- Mucinous Cystadenoma 0708Document12 pagesMucinous Cystadenoma 0708eosfieldNo ratings yet
- Gyne Long Exam 5 Premalignant and Malignant Lesions Vulva and VaginaDocument3 pagesGyne Long Exam 5 Premalignant and Malignant Lesions Vulva and VaginaRemelou Garchitorena AlfelorNo ratings yet
- SGH Cervical Screening Colposcopy PathwaysDocument13 pagesSGH Cervical Screening Colposcopy PathwaysAbraham ChiuNo ratings yet
- Distribuţia Genotipurilor Virusului Papiloma Uman La Paciente Din Zona MoldoveiDocument5 pagesDistribuţia Genotipurilor Virusului Papiloma Uman La Paciente Din Zona MoldoveiZama VitalieNo ratings yet
- Jurnal Vaksin HPVDocument9 pagesJurnal Vaksin HPVlitaayuningdyahNo ratings yet
- Pap TestDocument24 pagesPap TestAmirah MuhammadNo ratings yet
- Daftar Pustaka Kanker ServiksDocument3 pagesDaftar Pustaka Kanker ServiksRiri AmalinaNo ratings yet
- TNMC CreditDocument7 pagesTNMC CreditSathyaNo ratings yet
- CS-PUB-LAB-1 Cervical Cytology Management Recommendations Explanatory GuideDocument11 pagesCS-PUB-LAB-1 Cervical Cytology Management Recommendations Explanatory GuideMc Coral100% (1)
- Does Speculum Lubricant Affect Liquid Based Papanicolaou Test Adequacy?Document6 pagesDoes Speculum Lubricant Affect Liquid Based Papanicolaou Test Adequacy?Cristina CostaNo ratings yet
- Ovarian TumoursDocument41 pagesOvarian TumoursVlad RazvanNo ratings yet
- Cervical Pap Smear Study in a Tertiary HospitalDocument4 pagesCervical Pap Smear Study in a Tertiary HospitalkushalNo ratings yet
- 9 Endometrial Hyperplasia - Libre PathologyDocument5 pages9 Endometrial Hyperplasia - Libre PathologyfadoNo ratings yet
- Bethesda SystemDocument186 pagesBethesda SystemJoyce Pardo FernandezNo ratings yet
- HPV Vaksin 11 Maret 2023 - Dr. Cindy Rani SpOG KFER PDFDocument35 pagesHPV Vaksin 11 Maret 2023 - Dr. Cindy Rani SpOG KFER PDFYuliyanahNo ratings yet
- საშვ. ყელის ფონური დაავ-ბი IIDocument32 pagesსაშვ. ყელის ფონური დაავ-ბი IIAchi BeridzeNo ratings yet
- Hubungan Tingkat Pengetahuan Kanker Serviks Dengan Minat Untuk Vaksinasi HPV Pada Mahasiswi Fakultas Kedokteran Universitas HKBP Nommensen MedanDocument4 pagesHubungan Tingkat Pengetahuan Kanker Serviks Dengan Minat Untuk Vaksinasi HPV Pada Mahasiswi Fakultas Kedokteran Universitas HKBP Nommensen Medanintan fairuzNo ratings yet
- Bethesda system for reporting cervical cytologyDocument3 pagesBethesda system for reporting cervical cytologyNgotelo FunwiNo ratings yet