You might also like
- MOH Pocket Manual in Obstetrics and GynaecologyDocument194 pagesMOH Pocket Manual in Obstetrics and GynaecologyBea SamonteNo ratings yet
- Rtc-Scent 2012 05 Octaplex ProtocolDocument1 pageRtc-Scent 2012 05 Octaplex Protocolirene aureliaNo ratings yet
- AEMV 2009 Conference Full ProceedingsDocument66 pagesAEMV 2009 Conference Full Proceedingscristina_gomhNo ratings yet
- Case ReportDocument5 pagesCase ReportMira WardhaniNo ratings yet
- UHP ROTEM ImplementationDocument30 pagesUHP ROTEM Implementationppica8111No ratings yet
- Fluid Therapy - PICU Oct 2010 PDFDocument4 pagesFluid Therapy - PICU Oct 2010 PDFSiti ChodijahNo ratings yet
- Management of PPHDocument24 pagesManagement of PPHMutabazi SharifNo ratings yet
- DfneruigrDocument3 pagesDfneruigrKapy KapsNo ratings yet
- Oxytocin: The Hormone That Causes ContractionsDocument5 pagesOxytocin: The Hormone That Causes ContractionspreezaNo ratings yet
- Drugs Used in ObstetricsDocument21 pagesDrugs Used in Obstetricssuchismita panda100% (2)
- FDARDocument3 pagesFDARbeefy school onlyNo ratings yet
- MATERNITYDocument1 pageMATERNITYSanjie EufracioNo ratings yet
- Standing OrdersDocument27 pagesStanding OrdersDolly Sharma100% (2)
- Postpartal HemorrhageDocument54 pagesPostpartal HemorrhageInday BertaNo ratings yet
- Intrapartum fetal surveillanceDocument13 pagesIntrapartum fetal surveillanceamena mahmoudNo ratings yet
- Management of Postpartum Haemorrhage GuidelineDocument9 pagesManagement of Postpartum Haemorrhage GuidelineAyman A ArafatNo ratings yet
- Mid-trimester inductionDocument6 pagesMid-trimester inductionYwagar YwagarNo ratings yet
- Anaphylactic ReactionDocument12 pagesAnaphylactic Reactionelite100sprinter100% (1)
- Post Partum Haemorrhage (PPH)Document33 pagesPost Partum Haemorrhage (PPH)Khan WasimNo ratings yet
- Obstetric HaemorrhageDocument4 pagesObstetric Haemorrhageapi-142637023No ratings yet
- Fetal Blood Sampling: 1. PurposeDocument7 pagesFetal Blood Sampling: 1. PurposeMuathNo ratings yet
- Drug StudyDocument22 pagesDrug Studykit genitaNo ratings yet
- Neonatal Intensive Care RecordsDocument3 pagesNeonatal Intensive Care RecordsClaire LimosNo ratings yet
- MEDICAL MANAGEMENT OF POSTPARTUM HAEMORRHAGEDocument21 pagesMEDICAL MANAGEMENT OF POSTPARTUM HAEMORRHAGEFamilia Valdivia VilcaNo ratings yet
- Tambahan Utk Case ReportDocument4 pagesTambahan Utk Case ReportEdwin Batara SaragihNo ratings yet
- Managing Postpartum Hemorrhage (PPH) : Wisnu Prabowo DR Spog (KFM)Document43 pagesManaging Postpartum Hemorrhage (PPH) : Wisnu Prabowo DR Spog (KFM)christanto setiawanNo ratings yet
- Balloon Tamponade Uterine Pack PPH WCHN PPG 22052012Document5 pagesBalloon Tamponade Uterine Pack PPH WCHN PPG 22052012Achmad Safi'iNo ratings yet
- International Journal of Scientific Research: AnesthesiologyDocument2 pagesInternational Journal of Scientific Research: AnesthesiologyALfuNo ratings yet
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- SDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionDocument5 pagesSDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionYwagar YwagarNo ratings yet
- Cholecystitis CSDocument24 pagesCholecystitis CSMASII100% (1)
- MX of EclampsiaDocument5 pagesMX of EclampsiaYwagar YwagarNo ratings yet
- Drugs in ObstDocument32 pagesDrugs in ObstĶHwola ƏľsHokryNo ratings yet
- Obstetric Hemorrhage:: Intervening Safely and ExpeditiouslyDocument15 pagesObstetric Hemorrhage:: Intervening Safely and Expeditiouslyifa dhifaNo ratings yet
- Inotrope (Vasoactive Medication) Administration in The Paediatric Intensive Care Unit (PICU)Document6 pagesInotrope (Vasoactive Medication) Administration in The Paediatric Intensive Care Unit (PICU)Κατερίνα ΣιάλουNo ratings yet
- Nursing Care During Labor AND Birth: Group 3 - Ncma219RleDocument23 pagesNursing Care During Labor AND Birth: Group 3 - Ncma219Rlemonica mittiamNo ratings yet
- Management of Primary Postpartum HaemorrhageDocument16 pagesManagement of Primary Postpartum Haemorrhageapi-3705046100% (1)
- Guide to Epidural Use in LabourDocument11 pagesGuide to Epidural Use in LabourcignalNo ratings yet
- MgSO4 Therapy GuidelineDocument13 pagesMgSO4 Therapy GuidelineNisa UlfaturrosyidaNo ratings yet
- B4Y5G1 O - G - With AnswersDocument4 pagesB4Y5G1 O - G - With AnswersZeke EdgeNo ratings yet
- 06 Placenta Previa Revised Feb 06 PDFDocument4 pages06 Placenta Previa Revised Feb 06 PDFrendyNo ratings yet
- OptiLube Active Brochure 2012 Second EditionDocument4 pagesOptiLube Active Brochure 2012 Second EditionOptimum Medical SolutionsNo ratings yet
- 11 Drug StudyDocument13 pages11 Drug Studykwon nanaNo ratings yet
- Spontaneous Haemorrhagic Stroke Complicating Severe Pre-Eclampsia in Pregnancy: A Case Report in A Resource-Limited Setting in CameroonDocument4 pagesSpontaneous Haemorrhagic Stroke Complicating Severe Pre-Eclampsia in Pregnancy: A Case Report in A Resource-Limited Setting in CameroonDewina Dyani RosariNo ratings yet
- Blood transfusion cattleDocument3 pagesBlood transfusion cattlerajavet100% (1)
- Postpartal HemorrhageDocument9 pagesPostpartal HemorrhageJkimNo ratings yet
- Standard Operational Procedure PreeeclamsiaDocument4 pagesStandard Operational Procedure PreeeclamsiaDEBY SHINTANo ratings yet
- Emergency Peripartum Hysterectomy As Life Saving Surgery For Postpartum Haemorrhage in Women With Single Kidney - A CaseReportDocument5 pagesEmergency Peripartum Hysterectomy As Life Saving Surgery For Postpartum Haemorrhage in Women With Single Kidney - A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cesarean Hysterectomy With Cystotomy in Parturient Having Placenta Percreta, Gestational Thrombocytopenia, and Portal Hypertension - A Case ReportDocument4 pagesCesarean Hysterectomy With Cystotomy in Parturient Having Placenta Percreta, Gestational Thrombocytopenia, and Portal Hypertension - A Case ReportasclepiuspdfsNo ratings yet
- Maternity and Newborn MedicationsDocument38 pagesMaternity and Newborn MedicationsJaypee Fabros EdraNo ratings yet
- Understanding Postpartum Hemorrhage: Causes, Risks, Treatment and ManagementDocument30 pagesUnderstanding Postpartum Hemorrhage: Causes, Risks, Treatment and ManagementMuhamad IrsyadNo ratings yet
- Post Partum HemorrhageDocument59 pagesPost Partum HemorrhageMahima SharmaNo ratings yet
- Retained Placenta FinaleDocument5 pagesRetained Placenta FinaleJoy KirumbaNo ratings yet
- Drugs in PregnancyDocument52 pagesDrugs in Pregnancydarboeb265100% (2)
- Pharmacology Practice Test For NclexDocument10 pagesPharmacology Practice Test For NclexKira99% (96)
- Post Partum HemorrhageDocument12 pagesPost Partum HemorrhageMd. Lutfor Rahman KhanNo ratings yet
- Capture D'écran . 2023-07-20 À 11.16.50 PMDocument81 pagesCapture D'écran . 2023-07-20 À 11.16.50 PMWIDEDNo ratings yet
- P2010/0509-001 Management of EclampsiaDocument7 pagesP2010/0509-001 Management of EclampsiaYwagar YwagarNo ratings yet
- JINGCO - BSN 2-D - Module-6-Drug-StudyDocument16 pagesJINGCO - BSN 2-D - Module-6-Drug-StudyJashtine JingcoNo ratings yet
- Taper AssemblyDocument36 pagesTaper Assemblyויליאם סן מרמיגיוסNo ratings yet
- Approved List of Standards 30th March 2017Document13 pagesApproved List of Standards 30th March 2017adammzjinNo ratings yet
- 6005 Servo Tank GaugeDocument10 pages6005 Servo Tank GaugeadammzjinNo ratings yet
- Analytical Comparative Transport Cost Study On The Northern Corridor PDFDocument15 pagesAnalytical Comparative Transport Cost Study On The Northern Corridor PDFadammzjinNo ratings yet
- L T Piping Engineering 3 Day ProgremmeDocument352 pagesL T Piping Engineering 3 Day ProgremmenndhoreNo ratings yet
- Tec022 6000Document12 pagesTec022 6000nknicoNo ratings yet
- TDS 8127-Eng PDFDocument2 pagesTDS 8127-Eng PDFadammzjinNo ratings yet
- Report On South Sudan Market Survey PDFDocument29 pagesReport On South Sudan Market Survey PDFadammzjinNo ratings yet
- B31.3 Process Piping Course - 04 Pressure Design of MetalsDocument22 pagesB31.3 Process Piping Course - 04 Pressure Design of MetalsEryl YeongNo ratings yet
- Basic of PipingDocument64 pagesBasic of Pipingparameswaran shivakumar96% (46)
- Asme Viii CalcsDocument20 pagesAsme Viii CalcsSriram VjNo ratings yet
- National Foam Fire Fighting GuideDocument22 pagesNational Foam Fire Fighting Guidefloayzav5684100% (1)
- Hajj Umrah ChecklistDocument5 pagesHajj Umrah ChecklistadammzjinNo ratings yet
- Saturday, April 6, 2013 1330-1400 Hrs 1400-1600 Hrs. 1600-1630 Hrs. Venue: GTU Campus, Gandhinagar CampusDocument1 pageSaturday, April 6, 2013 1330-1400 Hrs 1400-1600 Hrs. 1600-1630 Hrs. Venue: GTU Campus, Gandhinagar CampusadammzjinNo ratings yet
- Jotamastic 80 Technical Data SheetDocument5 pagesJotamastic 80 Technical Data SheetNPTNo ratings yet
- ArgonLiquid390 29605Document1 pageArgonLiquid390 29605adammzjinNo ratings yet
- ANSI Flange RatingsDocument5 pagesANSI Flange Ratingssuperfly1984No ratings yet
- 3LPE Coating SpecificationDocument20 pages3LPE Coating SpecificationadammzjinNo ratings yet
- Shielding Gas Brochure410 80125Document32 pagesShielding Gas Brochure410 80125shaggerukNo ratings yet
- Hodge Clemco Ltd Vacuum Recovery System Replacement PartsDocument4 pagesHodge Clemco Ltd Vacuum Recovery System Replacement PartsadammzjinNo ratings yet
- Wasilatus ShafiDocument16 pagesWasilatus Shafiadammzjin100% (5)
- ANSI Flange RatingsDocument5 pagesANSI Flange Ratingssuperfly1984No ratings yet
- E194-837 - 842 Gases Conversion ChartDocument3 pagesE194-837 - 842 Gases Conversion ChartadammzjinNo ratings yet
- A Beginner's Guide To MIG WeldingDocument5 pagesA Beginner's Guide To MIG WeldingMIRCEA1305No ratings yet
- En Metalwork Gas Tungsten Arc WeldingDocument48 pagesEn Metalwork Gas Tungsten Arc WeldingadammzjinNo ratings yet
- Appendix G - Cryogenic Fluids-Weight and Volume EquivalentsDocument2 pagesAppendix G - Cryogenic Fluids-Weight and Volume EquivalentsadammzjinNo ratings yet
- Argon Liquid: Specification/gradeDocument1 pageArgon Liquid: Specification/gradeadammzjinNo ratings yet
- Appendix G - Cryogenic Fluids-Weight and Volume EquivalentsDocument2 pagesAppendix G - Cryogenic Fluids-Weight and Volume EquivalentsadammzjinNo ratings yet
- Product Data Sheet: Argon (Ar)Document2 pagesProduct Data Sheet: Argon (Ar)adammzjinNo ratings yet
- ConversionDocument2 pagesConversionadammzjinNo ratings yet
- Hiluf: EthiopiaDocument17 pagesHiluf: EthiopiaNewborn2013No ratings yet
- General Pathology MCQDocument3 pagesGeneral Pathology MCQSooPl33% (3)
- Data Interpretation For Medical Students PDFDocument905 pagesData Interpretation For Medical Students PDFMarNo ratings yet
- Hospital Staff, Equipment & DepartmentsDocument3 pagesHospital Staff, Equipment & DepartmentsHữu PhướcNo ratings yet
- Comparison of The Effect of Sectional Border Molding Using Different Molding and Final Impression Materials On The Retention of Maxillary Complete Denture BasesDocument6 pagesComparison of The Effect of Sectional Border Molding Using Different Molding and Final Impression Materials On The Retention of Maxillary Complete Denture BasesIOSRjournalNo ratings yet
- 123456789-Lectures On Homoeopathic Philosophy by JT Kent-123456789Document181 pages123456789-Lectures On Homoeopathic Philosophy by JT Kent-123456789fapatel95No ratings yet
- Introduction of Labour MonitoringDocument29 pagesIntroduction of Labour MonitoringMishti MokarramaNo ratings yet
- Abdominal Pain PDFDocument6 pagesAbdominal Pain PDFRandy MusashiNo ratings yet
- CHD Managemen Withot Surgery Cansy JHC (Prof. Mul) PDFDocument39 pagesCHD Managemen Withot Surgery Cansy JHC (Prof. Mul) PDFFery NurjayantoNo ratings yet
- Mortality Report April 25th 2019Document12 pagesMortality Report April 25th 2019ramotNo ratings yet
- A pictorial guide to key images in second trimester ultrasoundsDocument16 pagesA pictorial guide to key images in second trimester ultrasoundsSultan AlexandruNo ratings yet
- Peds Restorative PDFDocument4 pagesPeds Restorative PDFmirfanulhaqNo ratings yet
- Smart Solutions For OB/GYN: ACUSON X Family and ACUSON P Family Ultrasound SystemsDocument8 pagesSmart Solutions For OB/GYN: ACUSON X Family and ACUSON P Family Ultrasound SystemsPopescu ValiNo ratings yet
- The Hidden Face of EveDocument27 pagesThe Hidden Face of EveAna Julia PereiraNo ratings yet
- Caregiving Body TemperatureDocument69 pagesCaregiving Body TemperatureDanny Line100% (1)
- Appointment Details: NHS ConfidentialDocument2 pagesAppointment Details: NHS ConfidentialYash Vardhan DeoraNo ratings yet
- 019 Foot and Ankle ClassificationsDocument13 pages019 Foot and Ankle ClassificationsOh Deh100% (1)
- Hefler Et Al., 2009Document4 pagesHefler Et Al., 2009Jonathan LucisNo ratings yet
- Medical prescription abbreviation guideDocument10 pagesMedical prescription abbreviation guideFemi AlfarishiNo ratings yet
- Conyent Physiology of Third Stage of LabourDocument13 pagesConyent Physiology of Third Stage of LabourJay PaulNo ratings yet
- EntireDrugPack - BFN FINAL 090217 PDFDocument134 pagesEntireDrugPack - BFN FINAL 090217 PDFDeny HudaNo ratings yet
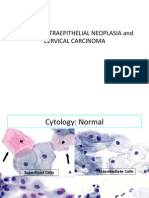
- 04 CIN and Cervical Cancer UNEDITEDDocument120 pages04 CIN and Cervical Cancer UNEDITEDRalph JuicoNo ratings yet
- CHN QuestionDocument4 pagesCHN QuestionSandeep KumarNo ratings yet
- Indian Public Health Standards (IPHS)Document2 pagesIndian Public Health Standards (IPHS)Nikcy N M NicklavoseNo ratings yet
- 7.dark Circles CausesDocument5 pages7.dark Circles CausesMohanraj VenuNo ratings yet
- Diagnosis and Management of Atypical Preeclampsia-Eclampsia: Obstetric Anesthesia Digest March 2010Document8 pagesDiagnosis and Management of Atypical Preeclampsia-Eclampsia: Obstetric Anesthesia Digest March 2010Fedrik Monte Kristo LimbongNo ratings yet
- Cerebral Palsy Guide to Types, Causes, Diagnosis and PrognosisDocument14 pagesCerebral Palsy Guide to Types, Causes, Diagnosis and PrognosisAfifah NaurahNo ratings yet
- How To Read A CTG - CTG InterpretationDocument45 pagesHow To Read A CTG - CTG InterpretationlicencaNo ratings yet
- Community Health NursingDocument9 pagesCommunity Health NursingtheglobalnursingNo ratings yet
- KIMS Board Discusses Reopening Plan and COVID-19 SOPsDocument6 pagesKIMS Board Discusses Reopening Plan and COVID-19 SOPsKIMS Malir CanttNo ratings yet