You might also like
- Compartment SyndromeDocument29 pagesCompartment SyndromeElla PriliandiniNo ratings yet
- Osteosarcoma - Docx (Recovered)Document25 pagesOsteosarcoma - Docx (Recovered)edhobiondiNo ratings yet
- Chang 2001Document4 pagesChang 2001edhobiondiNo ratings yet
- The Worldwide Prevalence of Methicillin-Resistant: Staphylococcus AureusDocument6 pagesThe Worldwide Prevalence of Methicillin-Resistant: Staphylococcus AureusedhobiondiNo ratings yet
- Elasfar 2013Document4 pagesElasfar 2013edhobiondiNo ratings yet
- Compartment Syndrome by Mary GasperDocument12 pagesCompartment Syndrome by Mary GasperedhobiondiNo ratings yet
- Swartz 1998Document6 pagesSwartz 1998jomoralesr91No ratings yet
- Hospital Disaster PlanDocument39 pagesHospital Disaster PlanRizki Puji AgustinNo ratings yet
- Mishima 1996Document3 pagesMishima 1996edhobiondiNo ratings yet
- Mini Camera User ManualDocument4 pagesMini Camera User ManualAndronikus Marintan NapitupuluNo ratings yet
- Complications of Pulmonary TuberculosisDocument18 pagesComplications of Pulmonary TuberculosisedhobiondiNo ratings yet
- Hospital Disaster PlanDocument39 pagesHospital Disaster PlanRizki Puji AgustinNo ratings yet
- PsikoterapiirDocument28 pagesPsikoterapiiredhobiondiNo ratings yet
- Psikoterapi 2Document9 pagesPsikoterapi 2edhobiondiNo ratings yet
- Huang 2014Document42 pagesHuang 2014edhobiondiNo ratings yet
- Somatoform and Sleep DisordersDocument18 pagesSomatoform and Sleep DisordersedhobiondiNo ratings yet
- Born As 2014Document8 pagesBorn As 2014edhobiondiNo ratings yet
- Heisel 2014Document12 pagesHeisel 2014edhobiondiNo ratings yet
- Somatoform and Sleep DisordersDocument18 pagesSomatoform and Sleep DisordersedhobiondiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 07a Scrutineering FSG Workshop Conti Hanover 20141018Document26 pages07a Scrutineering FSG Workshop Conti Hanover 20141018mc-andybroeker5182No ratings yet
- Times Leader 06-27-2011Document39 pagesTimes Leader 06-27-2011The Times LeaderNo ratings yet
- Electric Shocks and Electrocution, Clinical Effects and PathologyDocument9 pagesElectric Shocks and Electrocution, Clinical Effects and PathologyYosuaNo ratings yet
- Calisthenics Training Programs PDFDocument172 pagesCalisthenics Training Programs PDFKhalid SalimNo ratings yet
- Nerve Examination-Leprosy 2Document52 pagesNerve Examination-Leprosy 2Apriyani Supia DewiNo ratings yet
- Fall Protection Misconceptions and Myths PDFDocument18 pagesFall Protection Misconceptions and Myths PDFsebastian9033No ratings yet
- Jotungard Large RacesDocument16 pagesJotungard Large Racesfishguts4ever100% (10)
- A Treatise on Bone-Setting and Joint ManipulationDocument224 pagesA Treatise on Bone-Setting and Joint ManipulationChoo Kuan Wei100% (4)
- Atlas Shrugged - JeesiechreesieDocument231 pagesAtlas Shrugged - JeesiechreesieYaritza MirandaNo ratings yet
- Article Role of Zinc Post-Injury Wound Healing: Special inDocument3 pagesArticle Role of Zinc Post-Injury Wound Healing: Special inVinicio Rodriguez MirandaNo ratings yet
- Chest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehDocument54 pagesChest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehRayyan Alali100% (1)
- ww11701 Hunter - The - Reckoning + Vampire - The - Masquerade - Fiction - Predator - Prey - Book 2 - Judge PDFDocument288 pagesww11701 Hunter - The - Reckoning + Vampire - The - Masquerade - Fiction - Predator - Prey - Book 2 - Judge PDFPawel Vlad LatoNo ratings yet
- Spotters in Forensic MedicineDocument92 pagesSpotters in Forensic Medicines.misbaunnisa26100% (1)
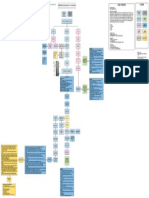
- Bone Fracture Concept MapDocument1 pageBone Fracture Concept MapJette Charmae OlboNo ratings yet
- Shoulder JointDocument6 pagesShoulder JointDr santoshNo ratings yet
- Intent to Kill Proven in Frustrated Homicide CaseDocument3 pagesIntent to Kill Proven in Frustrated Homicide CaseKara SolidumNo ratings yet
- Prehospital and Hospital Trauma CoordinationDocument4 pagesPrehospital and Hospital Trauma CoordinationnurulNo ratings yet
- Nursing Care in Plastic SurgeryDocument36 pagesNursing Care in Plastic Surgeryjengyee7186No ratings yet
- Chapter One (Ansci)Document19 pagesChapter One (Ansci)Yumie YamazukiNo ratings yet
- Bank Soalan MorfologiDocument12 pagesBank Soalan MorfologiwiesukhihotuNo ratings yet
- Chapter 2 Force and MotionDocument65 pagesChapter 2 Force and MotionAdsham100% (1)
- Dental Graft ProceduresDocument43 pagesDental Graft ProcedureskishanNo ratings yet
- BURNS SoftDocument3 pagesBURNS SoftErlo John Asentista0% (1)
- Sat Essential Grammar.38-40Document3 pagesSat Essential Grammar.38-40Tijana CurcicNo ratings yet
- DEMOLITIONHAMMERMANUALDocument14 pagesDEMOLITIONHAMMERMANUALIlia KiorlinskiNo ratings yet
- Pain Review PDFDocument770 pagesPain Review PDFmoisescharajaNo ratings yet
- ErgonomicsDocument21 pagesErgonomicsfayee123100% (1)
- Exercise Log AssignmentDocument25 pagesExercise Log Assignmentapi-300330301No ratings yet
- MC33883Document21 pagesMC33883Nguyen TuanNo ratings yet
- Knee Exam - OSCE Stations PDFDocument2 pagesKnee Exam - OSCE Stations PDFEmiel AwadNo ratings yet