You might also like
- Pancreatic Hormones Antidiabetic Drugs Part 2Document24 pagesPancreatic Hormones Antidiabetic Drugs Part 2jenet soleilNo ratings yet
- Oral Management of Diabetes Type IIDocument34 pagesOral Management of Diabetes Type IIYasser Gebril100% (1)
- British Journal of Diabetes & Vascular Disease-2013-Day-2-6Document6 pagesBritish Journal of Diabetes & Vascular Disease-2013-Day-2-6JrYounoezMuhammadNo ratings yet
- DM Emtyaz 3Document55 pagesDM Emtyaz 3Muhammed MuhsinNo ratings yet
- Meglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andDocument6 pagesMeglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andRifqoh Aulia AlthofunnisaNo ratings yet
- CKD Dan DM (Modul 4)Document6 pagesCKD Dan DM (Modul 4)Nurul AwaliahNo ratings yet
- 11 - Diabetes MellitusDocument63 pages11 - Diabetes MellitusShady ChapookNo ratings yet
- Diabetic Kidney Disease New Clinical and Therapeutic Issues Joint Position StatementDocument4 pagesDiabetic Kidney Disease New Clinical and Therapeutic Issues Joint Position StatementSiddiq MohammedNo ratings yet
- Pharmacological Management of Type 1 DiabetesDocument6 pagesPharmacological Management of Type 1 DiabetesMI RFNo ratings yet
- Drugs in Type 2 DMDocument18 pagesDrugs in Type 2 DMhussain AltaherNo ratings yet
- Diabetes PharmacologyDocument14 pagesDiabetes PharmacologyRich JeongNo ratings yet
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- Treatment of Diabetes MellitusDocument31 pagesTreatment of Diabetes MellitusIrfan IdealistNo ratings yet
- 4 Oral Hypoglycaemic DrugsDocument10 pages4 Oral Hypoglycaemic DrugsNashat SaadiNo ratings yet
- Spesialits Obat Diabetes MellitusDocument18 pagesSpesialits Obat Diabetes MellitusmaudynurrNo ratings yet
- Cleveland Clinic Journal of Medicine 2009 SHRISHRIMAL 649 55Document7 pagesCleveland Clinic Journal of Medicine 2009 SHRISHRIMAL 649 55คุณนาย เหม่เกว่No ratings yet
- ANTIDIABETICSDocument25 pagesANTIDIABETICSkookiescream100% (2)
- Metformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetDocument11 pagesMetformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetAfifa ZainNo ratings yet
- Sulfonylurea Pharmacology Updates 2020Document3 pagesSulfonylurea Pharmacology Updates 2020AHMED TANJIMUL ISLAMNo ratings yet
- FR H 6788 001 FinalSPCDocument28 pagesFR H 6788 001 FinalSPCabenezer g/kirstosNo ratings yet
- MetFormin Generic Health TabDocument9 pagesMetFormin Generic Health TabNur Ekayani SyamNo ratings yet
- Pharmacotherapy of Diabetes MellitusDocument32 pagesPharmacotherapy of Diabetes MellitusGhilli Jaya PrakashNo ratings yet
- Glycemia and Kidney RDocument27 pagesGlycemia and Kidney RMARIA VICTORIA VELARDE ALIAGANo ratings yet
- Pharmacologic TheraphyDocument32 pagesPharmacologic TheraphyquinnNo ratings yet
- Saxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsDocument11 pagesSaxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsLaura MelatiNo ratings yet
- Diabetes Mellitus - UG NotesDocument10 pagesDiabetes Mellitus - UG NotesRayan ElRasheedNo ratings yet
- Endo Pharma ElhDocument14 pagesEndo Pharma Elhodiodi57No ratings yet
- Diabetes Mellitus Type 2Document42 pagesDiabetes Mellitus Type 2alexandrajane2007No ratings yet
- Pharmacological Treatment: Type 1 Diabetes Mellitus Type 2 Diabetes MellitusDocument26 pagesPharmacological Treatment: Type 1 Diabetes Mellitus Type 2 Diabetes Mellitusiron100% (1)
- Jardiance Epar Product Information - enDocument47 pagesJardiance Epar Product Information - enSaad MasoodNo ratings yet
- ADO1 Agst 2013Document48 pagesADO1 Agst 2013blackjackNo ratings yet
- Tatalaksana Diabetes Pada Pelayanan PrimerDocument49 pagesTatalaksana Diabetes Pada Pelayanan PrimerEvri LiaNo ratings yet
- Drug StudyDocument13 pagesDrug StudyAllan DiazNo ratings yet
- 02 - Update Article New Oral Antidiabetic AgentsDocument7 pages02 - Update Article New Oral Antidiabetic AgentsMuhammad Lutfi Al AyubiNo ratings yet
- L Tiple: Përgjigje-Kumar&Clark 'S Clinical MedicineDocument10 pagesL Tiple: Përgjigje-Kumar&Clark 'S Clinical MedicineNreca TokjonaNo ratings yet
- Diabetes AssignmentDocument8 pagesDiabetes AssignmentMildred Obeng AgyeiwaaNo ratings yet
- Metformin Hydrochloride PDFDocument4 pagesMetformin Hydrochloride PDFHannaNo ratings yet
- Drug Management of Diabetes MellitusDocument36 pagesDrug Management of Diabetes MellitusHassan.shehri100% (15)
- 07-Anti Diabetes DrugsDocument12 pages07-Anti Diabetes Drugsraginivermaa20No ratings yet
- Insulin PharmacologyDocument4 pagesInsulin PharmacologySunilNo ratings yet
- Oral Antidiabetics in Specific ConditionsDocument3 pagesOral Antidiabetics in Specific Conditionsbelahan jiwaNo ratings yet
- Kuliah 5. Kasus 1 Dan 2 (GGK)Document94 pagesKuliah 5. Kasus 1 Dan 2 (GGK)yudiNo ratings yet
- L87 - Oral Hypoglycemic AgentsDocument17 pagesL87 - Oral Hypoglycemic AgentsalijanmarwatNo ratings yet
- Classifications of Insulin2Document116 pagesClassifications of Insulin2loglesb1No ratings yet
- Makalah Modul VIIDocument33 pagesMakalah Modul VIILeen NisNo ratings yet
- 08&09 Oral Hypoglycemics-Level 11Document48 pages08&09 Oral Hypoglycemics-Level 11Usman Ali AkbarNo ratings yet
- Diabetes Mellitus (DM) : ContentDocument30 pagesDiabetes Mellitus (DM) : ContentMompati LetsweletseNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Drugs and Kidney DiseasesDocument46 pagesDrugs and Kidney Diseasesمرتضى محمد فاضل جرجوكNo ratings yet
- HypoglycemiaDocument19 pagesHypoglycemiaJesus PadillaNo ratings yet
- Diabetes MedicationDocument17 pagesDiabetes MedicationTaj lamajedNo ratings yet
- Anti Diabetic DrugDocument45 pagesAnti Diabetic DrugRahul LokhandeNo ratings yet
- Glucovance Tablet Salut Selaput 500 mg-5 MG - Metformin Hidroklorida-Glibenclaminde - DKL1715809217C1 - 2021 - 0Document16 pagesGlucovance Tablet Salut Selaput 500 mg-5 MG - Metformin Hidroklorida-Glibenclaminde - DKL1715809217C1 - 2021 - 0Felesia MissyNo ratings yet
- Approach ConsiderationsDocument12 pagesApproach ConsiderationsTyna Mew-mewNo ratings yet
- Dipeptidyl Peptidase-4 (Dpp-4) Inhibitors in The Management of DiabetesDocument6 pagesDipeptidyl Peptidase-4 (Dpp-4) Inhibitors in The Management of DiabetesDr. PanditNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDocument6 pagesLewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDeo FactuarNo ratings yet
- Drugs Involving Blood GlucoseDocument23 pagesDrugs Involving Blood GlucoseMary Faith Kiat-ongNo ratings yet
- Lec 1Document9 pagesLec 1fbbqbcht6yNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Coagulation Cascade: Difference Between Intrinsic and Extrinsic PathwayDocument10 pagesCoagulation Cascade: Difference Between Intrinsic and Extrinsic Pathwayroshmae100% (1)
- IM - Focal Seizure ReportDocument2 pagesIM - Focal Seizure ReportroshmaeNo ratings yet
- Cap PDFDocument1 pageCap PDFroshmaeNo ratings yet
- CPG Pcap 2012 PDFDocument54 pagesCPG Pcap 2012 PDFroshmae67% (3)
- FCM IiiDocument2 pagesFCM IiiroshmaeNo ratings yet
- Topic:: Obejctives Content TA T-L Activitie S Materials Resources Evaluatio NDocument2 pagesTopic:: Obejctives Content TA T-L Activitie S Materials Resources Evaluatio NroshmaeNo ratings yet
- BP: HR: RR: Temp:: CBC Count Pulse Oximetry (Oxygen Saturation) CreatinineDocument2 pagesBP: HR: RR: Temp:: CBC Count Pulse Oximetry (Oxygen Saturation) CreatinineroshmaeNo ratings yet
- Sentinel Lymph Node DissectionDocument9 pagesSentinel Lymph Node DissectionroshmaeNo ratings yet
- HypothyroidismDocument3 pagesHypothyroidismroshmaeNo ratings yet
- Gyne - Functional Ovarian Cysts Treatment and ManagementDocument1 pageGyne - Functional Ovarian Cysts Treatment and ManagementroshmaeNo ratings yet
- Precipitating Factors: Predisposing FactorsDocument1 pagePrecipitating Factors: Predisposing FactorsroshmaeNo ratings yet
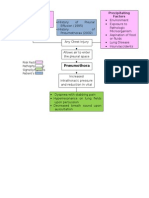
- Pneumothora X: Precipitating Factors Predisposing FactorsDocument1 pagePneumothora X: Precipitating Factors Predisposing FactorsroshmaeNo ratings yet
- PD - Heart Failure ReportDocument28 pagesPD - Heart Failure ReportroshmaeNo ratings yet
- Gyne - Torsion of Dermoid CystDocument4 pagesGyne - Torsion of Dermoid CystroshmaeNo ratings yet
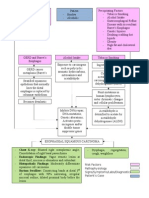
- Pathophysiology of Esophageal CADocument2 pagesPathophysiology of Esophageal CAroshmae100% (4)
- FLG 212 Study GuideDocument19 pagesFLG 212 Study GuidecynthiaNo ratings yet
- DH VSCC Intern Manual 4th Edition - WEB PDFDocument124 pagesDH VSCC Intern Manual 4th Edition - WEB PDFXyzNo ratings yet
- Child Guidance ClinicDocument22 pagesChild Guidance ClinicBinal Joshi67% (3)
- Board EamDocument55 pagesBoard Eamjoycevillamor100% (1)
- Assessment of Abnormal Behaviour: Lindsay Ayearst, PH.DDocument32 pagesAssessment of Abnormal Behaviour: Lindsay Ayearst, PH.DMagishaa ThiyagarajahNo ratings yet
- NearfatalasthmaDocument8 pagesNearfatalasthmaHeath HensleyNo ratings yet
- DARUNDAY - NCM 117 Asynchronous ActivityDocument17 pagesDARUNDAY - NCM 117 Asynchronous ActivityEzra Miguel DarundayNo ratings yet
- Cold Agglutinin DiseaseDocument4 pagesCold Agglutinin Diseasenavneet21usNo ratings yet
- OB Midwifery Set 1 PDFDocument9 pagesOB Midwifery Set 1 PDFSquidward Tentacles100% (1)
- Risk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesDocument6 pagesRisk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesRendra SyaniNo ratings yet
- Hyperbaric Oxygen Therapy: ReferenceDocument5 pagesHyperbaric Oxygen Therapy: ReferenceFariz NurNo ratings yet
- Case Study Intramedullary Spinal Cord TumorDocument13 pagesCase Study Intramedullary Spinal Cord TumorCitra KristiNo ratings yet
- DiclofenacDocument3 pagesDiclofenacapi-37979410% (1)
- Clinical Pharmacy - Introduction - : Prepared By: Dr. C. Suhas ReddyDocument20 pagesClinical Pharmacy - Introduction - : Prepared By: Dr. C. Suhas Reddysuhas reddyNo ratings yet
- TriageDocument30 pagesTriageJairo Andres Rueda MartinezNo ratings yet
- Factitious DisorderDocument6 pagesFactitious Disorderayu yuliantiNo ratings yet
- Pharmaceutical CareDocument114 pagesPharmaceutical CareRisdaFitriaNo ratings yet
- Congenital Syphilis Treatment and PreventionDocument1 pageCongenital Syphilis Treatment and PreventionMuhammad Naufal FadhillahNo ratings yet
- Treatment Dysarthria EfficacyDocument12 pagesTreatment Dysarthria EfficacySwathi GeethaNo ratings yet
- MRNA VaccineDocument23 pagesMRNA VaccineIsworo RukmiNo ratings yet
- Case Presentation of DepressionDocument39 pagesCase Presentation of DepressionHeden Collado100% (1)
- Test Bank Alexanders Care of The Patient in Surgery 16th Edition RothrockDocument4 pagesTest Bank Alexanders Care of The Patient in Surgery 16th Edition RothrockCarlton Caughey100% (34)
- Blood Donation RequirementsDocument29 pagesBlood Donation RequirementsMaria Cecilia FloresNo ratings yet
- Sarcoidosis y UveitisDocument10 pagesSarcoidosis y UveitisJavier Infantes MolinaNo ratings yet
- Wound Care Procedure StudentsDocument2 pagesWound Care Procedure StudentsJan Philippe BelandoNo ratings yet
- Bimanual Vaginal Examination - OSCE Guide - Geeky MedicsDocument6 pagesBimanual Vaginal Examination - OSCE Guide - Geeky MedicsJahangir AlamNo ratings yet
- Pathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationDocument1 pagePathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationAzhar SabriNo ratings yet
- Clock Drawing TestDocument5 pagesClock Drawing TestrumaishaNo ratings yet
- B Scan Ultrasonography01Document54 pagesB Scan Ultrasonography01dr samreen arif50% (2)