You might also like
- Cranial Nerve Nuclei and Their FunctionsDocument6 pagesCranial Nerve Nuclei and Their FunctionsThanat PetchrodNo ratings yet
- Pituitary Adenoma Classification, Presentation, and TreatmentDocument20 pagesPituitary Adenoma Classification, Presentation, and TreatmentAbdulaziz Al-TaisanNo ratings yet
- Eating Disorder Anorexia Nervosa ExplainedDocument21 pagesEating Disorder Anorexia Nervosa ExplainedIndah Permata SariNo ratings yet
- PsychosisDocument32 pagesPsychosisRamya Gopala KrishnanNo ratings yet
- Terms in The Field of PsychiatryDocument18 pagesTerms in The Field of PsychiatryOchie YecyecanNo ratings yet
- DR - Usama.mahmoud Psychiatry - Notes MSDocument64 pagesDR - Usama.mahmoud Psychiatry - Notes MSMariam A. KarimNo ratings yet
- Psych Ch. 5 NotesDocument7 pagesPsych Ch. 5 NotesHaylle ThomasNo ratings yet
- Case Study 142: Assessing Suicide Risk in a Depressed Elderly PatientDocument5 pagesCase Study 142: Assessing Suicide Risk in a Depressed Elderly PatientPatricia Ann Nicole ReyesNo ratings yet
- Effect of Aripiprazole Augmentation of Clozapine in SchizophreniaDocument28 pagesEffect of Aripiprazole Augmentation of Clozapine in SchizophreniaamaldutaNo ratings yet
- Increased ICP: A) HeadacheDocument5 pagesIncreased ICP: A) Headachemohamed nagyNo ratings yet
- Psychiatry Notes - Depressive DisorderDocument2 pagesPsychiatry Notes - Depressive DisorderLiSenNo ratings yet
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Anxiety and Psychosexual Disorders in ChildDocument60 pagesAnxiety and Psychosexual Disorders in ChildAnnalesa BarkerNo ratings yet
- Clinical Features of Common Psychiatric DisordersDocument21 pagesClinical Features of Common Psychiatric DisordersShivan A.C.No ratings yet
- Overview of Psychotropic DrugsDocument7 pagesOverview of Psychotropic Drugsnad101No ratings yet
- Brain Imaging in PsychiatryDocument7 pagesBrain Imaging in PsychiatryKaram Ali ShahNo ratings yet
- Neurodegenerative disorders and their managementDocument61 pagesNeurodegenerative disorders and their managementMarites Santos AquinoNo ratings yet
- Psychiatry Student Guide: MEDD 421 Clinical Skills 2019-2020Document25 pagesPsychiatry Student Guide: MEDD 421 Clinical Skills 2019-2020Rubie Ann TillorNo ratings yet
- PHARMACOLOGY OF PSYCHOSIS AND MANIADocument53 pagesPHARMACOLOGY OF PSYCHOSIS AND MANIAlavanyakakarlaNo ratings yet
- Neurodevelopmental Disorders FinalDocument7 pagesNeurodevelopmental Disorders FinalAARON JOHN VIRAYNo ratings yet
- MC IIIA Topics: Midterm Material. Won't Be in The Final Exam, Only Antiparkinsonian IncludedDocument138 pagesMC IIIA Topics: Midterm Material. Won't Be in The Final Exam, Only Antiparkinsonian IncludedToqa ElmansouryNo ratings yet
- Anxiety Disorders: Types, Symptoms, and TreatmentsDocument62 pagesAnxiety Disorders: Types, Symptoms, and TreatmentsPRHSTNo ratings yet
- Neuroleptic Advers ReactionDocument65 pagesNeuroleptic Advers Reactionayu yulianti100% (1)
- Roadmap to a Psychiatric Residency CareerDocument21 pagesRoadmap to a Psychiatric Residency Careercatalin_ilie_5No ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801No ratings yet
- Epilepsy Mechanisms and Treatment OptionsDocument49 pagesEpilepsy Mechanisms and Treatment OptionsIe Dochie100% (1)
- Psych Ch. 7 Notes (Tutor)Document5 pagesPsych Ch. 7 Notes (Tutor)Haylle ThomasNo ratings yet
- Diagnosing Mental DisordersDocument4 pagesDiagnosing Mental DisordersdrqubitNo ratings yet
- Understanding Antipsychotic DrugsDocument22 pagesUnderstanding Antipsychotic DrugsvinodksahuNo ratings yet
- Vascular DementiaDocument5 pagesVascular DementiaAna Ramos LopezNo ratings yet
- Buku Comprehensive Textbook PsychiatryDocument76 pagesBuku Comprehensive Textbook PsychiatryHadi GunaNo ratings yet
- Behavioral FinalsDocument28 pagesBehavioral FinalsKofiBNo ratings yet
- Delirium and Its ManagmentDocument64 pagesDelirium and Its ManagmentViren Solanki100% (1)
- Week 10 - Hypertension, Atherosclerosis, ArrhythmiaDocument14 pagesWeek 10 - Hypertension, Atherosclerosis, Arrhythmiashivani patel100% (1)
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyD. W. S JayarathnaNo ratings yet
- INTRODUCTION TO NEUROPHARMACOLOGYyyDocument27 pagesINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviNo ratings yet
- Obat-Obat Psychiatry - 1 2018Document104 pagesObat-Obat Psychiatry - 1 2018Christo LimbongNo ratings yet
- Basal Ganglia: Sridharan Neelamegan MMCDocument23 pagesBasal Ganglia: Sridharan Neelamegan MMCRetrocasualty Find OutNo ratings yet
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocument8 pagesCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNo ratings yet
- Epidemiological Data: Paper B Syllabic Content 7.xDocument5 pagesEpidemiological Data: Paper B Syllabic Content 7.xAnamika SinhaNo ratings yet
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- Psychiatry Notes - Defenses MechanismsDocument2 pagesPsychiatry Notes - Defenses MechanismsLiSenNo ratings yet
- Treatment Resistant OCD .Document55 pagesTreatment Resistant OCD .Dr viren SolankiNo ratings yet
- Neuroleptic Malignant Syndrome MedscapeDocument9 pagesNeuroleptic Malignant Syndrome MedscapeEra SulistiyaNo ratings yet
- TrOn ReferencesDocument11 pagesTrOn ReferencesAnonymous CbnCgjNo ratings yet
- MCQ I II Psych 2 PDFDocument19 pagesMCQ I II Psych 2 PDFSpacetoon DaysNo ratings yet
- Guide to Antipsychotics for SchizophreniaDocument24 pagesGuide to Antipsychotics for SchizophreniaKhadija ArshadNo ratings yet
- AnticholinergicDocument16 pagesAnticholinergicLily CentenoNo ratings yet
- Medicines in PregnancyDocument18 pagesMedicines in Pregnancymominur11No ratings yet
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatNo ratings yet
- Case Study 5 - 8 - PsychosisDocument17 pagesCase Study 5 - 8 - PsychosisanojanNo ratings yet
- Types of DepressionDocument12 pagesTypes of DepressionKADAMBARINo ratings yet
- Antiepileptics (Autosaved)Document57 pagesAntiepileptics (Autosaved)vishal singhNo ratings yet
- Biochemistry of neurotransmittersDocument19 pagesBiochemistry of neurotransmittersKate TaylorNo ratings yet
- Diagnosing Secondary Headaches (Practical Neurology) (2020 - 05)Document5 pagesDiagnosing Secondary Headaches (Practical Neurology) (2020 - 05)Apostolos T.No ratings yet
- Traumatic Brain InjuryDocument88 pagesTraumatic Brain Injurympm8471No ratings yet
- Pediatrics: St. Elizabeth Family Medicine Residency ProgramDocument9 pagesPediatrics: St. Elizabeth Family Medicine Residency Programwingchun108tekNo ratings yet
- Cardio Day 3: Hypertension, Hyperlipidemia, Arteriosclerosis, Ischemic Heart DiseaseDocument24 pagesCardio Day 3: Hypertension, Hyperlipidemia, Arteriosclerosis, Ischemic Heart DiseaseMikeNo ratings yet
- ECTDocument24 pagesECTEdgar ManoodNo ratings yet
- Errors in Metabolism BiochemsmallDocument1 pageErrors in Metabolism BiochemsmallTeresa MartinsNo ratings yet
- Lit SkinStruct Bensouillah Ch01 PDFDocument11 pagesLit SkinStruct Bensouillah Ch01 PDFisaco1531012No ratings yet
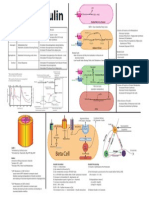
- Intro To InsulinDocument1 pageIntro To InsulinTeresa MartinsNo ratings yet
- Blood supply and hormone secretion in the islets of LangerhansDocument1 pageBlood supply and hormone secretion in the islets of LangerhansTeresa MartinsNo ratings yet
- Virchows TriadDocument1 pageVirchows TriadTeresa MartinsNo ratings yet
- Adrenal and ParathyroidDocument1 pageAdrenal and ParathyroidTeresa MartinsNo ratings yet
- Thoracic AnatomyDocument1 pageThoracic AnatomyTeresa Martins100% (1)
- Ekg MorphologyDocument1 pageEkg MorphologyTeresa MartinsNo ratings yet
- Vascular Function CurveDocument1 pageVascular Function CurveTeresa MartinsNo ratings yet
- Growth Chart Tool DevoDocument1 pageGrowth Chart Tool DevoTeresa MartinsNo ratings yet
- Ekg PracticeDocument1 pageEkg PracticeTeresa MartinsNo ratings yet
- Overview of Metabolism: Glucose Alanine CycleDocument1 pageOverview of Metabolism: Glucose Alanine CycleTeresa MartinsNo ratings yet
- Cardiac Glycosides Improve Heart Failure by Increasing Calcium ReuptakeDocument1 pageCardiac Glycosides Improve Heart Failure by Increasing Calcium ReuptakeTeresa MartinsNo ratings yet
- Cardiac Action PotentialsDocument1 pageCardiac Action PotentialsTeresa MartinsNo ratings yet
- Behavioral Science TimelinesmallDocument1 pageBehavioral Science TimelinesmallTeresa MartinsNo ratings yet
- Cell CycleDocument1 pageCell CycleTeresa MartinsNo ratings yet
- Overview of Psych DisordersDocument4 pagesOverview of Psych DisordersTeresa MartinsNo ratings yet
- Characterization of Foxo3a-Mediated Gene Expression Following Bez ExposureDocument9 pagesCharacterization of Foxo3a-Mediated Gene Expression Following Bez ExposureTeresa MartinsNo ratings yet
- Overview of Psych DisordersDocument4 pagesOverview of Psych DisordersTeresa MartinsNo ratings yet
- MEE Teresa Martins A39062Document15 pagesMEE Teresa Martins A39062Teresa MartinsNo ratings yet
- Characterization of Foxo3a-Mediated Gene Expression Following Bez ExposureDocument9 pagesCharacterization of Foxo3a-Mediated Gene Expression Following Bez ExposureTeresa MartinsNo ratings yet
- Application - Form-ESN FaroDocument4 pagesApplication - Form-ESN FaroTeresa MartinsNo ratings yet
- MEE Teresa Martins A39062Document15 pagesMEE Teresa Martins A39062Teresa MartinsNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)Document26 pagesNonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)ROHITNo ratings yet
- Anxiety 2Document11 pagesAnxiety 2tela teliNo ratings yet
- AAPCDocument10 pagesAAPCprincyphilip67% (3)
- Main ICM Shelf Exam (2012 Nov MUA)Document8 pagesMain ICM Shelf Exam (2012 Nov MUA)mentawistNo ratings yet
- Interstitial Lung DiseasesDocument80 pagesInterstitial Lung Diseasespavithranmbbs100% (1)
- Principles and Practice of Implant Dentistry 2001 - Weiss (18-15)Document671 pagesPrinciples and Practice of Implant Dentistry 2001 - Weiss (18-15)Paulo Carvalho100% (2)
- NCP Submucous MyomaDocument1 pageNCP Submucous MyomaRichmon VillaminNo ratings yet
- q1 Exam - RESEARCH IIDocument6 pagesq1 Exam - RESEARCH IIjohnry colmenaresNo ratings yet
- Anatomy and Physiology 6th Edition Marieb Solutions Manual DownloadDocument11 pagesAnatomy and Physiology 6th Edition Marieb Solutions Manual DownloadKatie Herrera100% (26)
- Neuroendocrine Tumors Dr. WarsinggihDocument20 pagesNeuroendocrine Tumors Dr. WarsinggihAndi Eka Putra PerdanaNo ratings yet
- Drowning: DR K.B.Suryakumar Prof & HOD Dept of Forensic Medicine KVG Medical College Sullia - KarnatakaDocument33 pagesDrowning: DR K.B.Suryakumar Prof & HOD Dept of Forensic Medicine KVG Medical College Sullia - KarnatakaSuryakumar KilarNo ratings yet
- Module 4 - Applying Basic First AidDocument2 pagesModule 4 - Applying Basic First AidjessafesalazarNo ratings yet
- Excision of Branchial CystDocument9 pagesExcision of Branchial CystMeddco dicoveredNo ratings yet
- PRSG Officer Candidate Application FormDocument12 pagesPRSG Officer Candidate Application FormJesus E. Delgado33% (3)
- Nutrition Myths BustedDocument2 pagesNutrition Myths BustedNoob KidNo ratings yet
- Clitoridectomy: A Nineteenth Century Answer To Masturbation by JohnDocument3 pagesClitoridectomy: A Nineteenth Century Answer To Masturbation by JohnthewomenofislamNo ratings yet
- A 75 Year-Old Male With Obstructive Jaundice and A Pancreatic Head MassDocument8 pagesA 75 Year-Old Male With Obstructive Jaundice and A Pancreatic Head MasssilcmtgNo ratings yet
- AlbendazoleDocument7 pagesAlbendazolefinchan IrawanNo ratings yet
- Enterocutaneous FistulaDocument37 pagesEnterocutaneous FistulaAdityadewi SulistyoNo ratings yet
- Adult PSG Guidelines 2014Document49 pagesAdult PSG Guidelines 2014mohanNo ratings yet
- Seeleys Anatomy Physiology 10th Edition Test Bank Cinnamon VanputteDocument61 pagesSeeleys Anatomy Physiology 10th Edition Test Bank Cinnamon VanputteHorace Samuel100% (27)
- Grain & Oil Science and Technology: Balasubramaniam Jaya Prasad, Pazhaniyandi Subramania Sharavanan, Rengaraj SivarajDocument5 pagesGrain & Oil Science and Technology: Balasubramaniam Jaya Prasad, Pazhaniyandi Subramania Sharavanan, Rengaraj SivarajYahya SudrajatNo ratings yet
- 8 Nursing Care of A Postpartal Family and FamilyDocument41 pages8 Nursing Care of A Postpartal Family and FamilyJelly Yanquiling DumlaoNo ratings yet
- Bacterial Vaginosis - IntanDocument9 pagesBacterial Vaginosis - IntanIntan Noor NaqiahNo ratings yet
- DNA RepairDocument35 pagesDNA RepairAbid Al RezaNo ratings yet
- Clinical Concept MapDocument16 pagesClinical Concept MapEric MillsNo ratings yet
- Ultrasonography of The EyeDocument8 pagesUltrasonography of The Eyetaner_soysurenNo ratings yet
- Aparato Urogenital 2018 PDFDocument66 pagesAparato Urogenital 2018 PDFCJ CANo ratings yet
- Use of Dr. Tans Chinese Balance AcupunctDocument9 pagesUse of Dr. Tans Chinese Balance AcupunctrendaoNo ratings yet
- Parotid Gland AnatomyDocument24 pagesParotid Gland AnatomykeerthanaNo ratings yet