You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Taylor 5563 Scale 5563 ManualDocument2 pagesTaylor 5563 Scale 5563 ManualNick Visutsithiwong0% (1)
- A Study of Menstrual Distress Questionnaire in First Year Medical StudentsDocument4 pagesA Study of Menstrual Distress Questionnaire in First Year Medical StudentswidyaersafitriNo ratings yet
- Factors Affecting Wound HealingDocument11 pagesFactors Affecting Wound HealingFredy Rodeardo MaringgaNo ratings yet
- Manual DentalclinicDocument47 pagesManual DentalclinicjugnuNo ratings yet
- Total Joint ReplacementDocument2 pagesTotal Joint ReplacementjugnuNo ratings yet
- Radiology Templates For WebsiteDocument4 pagesRadiology Templates For WebsitejugnuNo ratings yet
- VitaminsDocument17 pagesVitaminsjugnuNo ratings yet
- 2008 - Carol Anne Murdoch Kinch - DoseEffectRelationshipsfortheSubmandibularSalivaryretrieved-2015!07!04Document10 pages2008 - Carol Anne Murdoch Kinch - DoseEffectRelationshipsfortheSubmandibularSalivaryretrieved-2015!07!04jugnuNo ratings yet
- An Update On Demineralization/Remineralization: Mark E. Jensen, MS, DDS, PHD Robert V. Faller, BsDocument29 pagesAn Update On Demineralization/Remineralization: Mark E. Jensen, MS, DDS, PHD Robert V. Faller, BsjugnuNo ratings yet
- Ce 376Document14 pagesCe 376AdiNo ratings yet
- Technical Manual Written OSCE AFK ACJ - 2012 Public Version WEBDocument41 pagesTechnical Manual Written OSCE AFK ACJ - 2012 Public Version WEBjugnuNo ratings yet
- ACJ Course DescriptionDocument2 pagesACJ Course DescriptionjugnuNo ratings yet
- Dverse Reactions To Latex ProductsDocument17 pagesDverse Reactions To Latex ProductsjugnuNo ratings yet
- Newsletter 11 10Document4 pagesNewsletter 11 10jugnuNo ratings yet
- BibliographyDocument2 pagesBibliographyjugnuNo ratings yet
- Ce 301Document18 pagesCe 301jugnuNo ratings yet
- Introductions - Slide 1Document1 pageIntroductions - Slide 1jugnuNo ratings yet
- Oil Sands: Economy/Pages/what-are-oilsands - AspxDocument5 pagesOil Sands: Economy/Pages/what-are-oilsands - AspxjugnuNo ratings yet
- Political Legal EnvironmentDocument1 pagePolitical Legal EnvironmentjugnuNo ratings yet
- Harper Corp Wheat Harvest Ops Year 1 FinancialsDocument2 pagesHarper Corp Wheat Harvest Ops Year 1 Financialsjugnu0% (1)
- End Notes (Chicago Style)Document2 pagesEnd Notes (Chicago Style)jugnuNo ratings yet
- Spring CoursesDocument59 pagesSpring CoursesjugnuNo ratings yet
- Political Legal EnvironmentDocument1 pagePolitical Legal EnvironmentjugnuNo ratings yet
- Financial ForecastingDocument15 pagesFinancial ForecastingjugnuNo ratings yet
- Oil SandsDocument28 pagesOil SandsjugnuNo ratings yet
- MCQs on Depreciation AccountingDocument3 pagesMCQs on Depreciation AccountingjugnuNo ratings yet
- Business Communication: Subject Code - Bcom12Document2 pagesBusiness Communication: Subject Code - Bcom12jugnuNo ratings yet
- (DD13-14) Dental AnatomyDocument443 pages(DD13-14) Dental AnatomyJacobsen RichardNo ratings yet
- The GPHC Question List Jun17-Mch21Document35 pagesThe GPHC Question List Jun17-Mch21Patrick MathewNo ratings yet
- CPE 103 Lecture on Developmental DisabilitiesDocument29 pagesCPE 103 Lecture on Developmental DisabilitiesMay Flor T. BelandoNo ratings yet
- M1 Introduction To EpidemiologyDocument3 pagesM1 Introduction To EpidemiologyMc Philip Gabay DamoclesNo ratings yet
- Drug Study - CeftizidimeDocument2 pagesDrug Study - CeftizidimeRay Daniel E. BilbaoNo ratings yet
- Burnout Syndrome - Stress in Health Care Professionals Working To Fight Covid-19 in Public HospitalsDocument14 pagesBurnout Syndrome - Stress in Health Care Professionals Working To Fight Covid-19 in Public HospitalsIJAERS JOURNALNo ratings yet
- Module On Gecsel: Understanding The SelfDocument42 pagesModule On Gecsel: Understanding The SelfJpoy RiveraNo ratings yet
- Rectovagina FistulaDocument13 pagesRectovagina FistulaNurul HikmahNo ratings yet
- History of Polio-1Document21 pagesHistory of Polio-1world photocopyNo ratings yet
- Nursing Questions on Gastrointestinal DisordersDocument11 pagesNursing Questions on Gastrointestinal DisordersA SungNo ratings yet
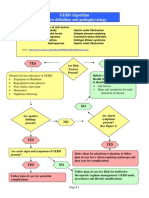
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Cattle RaisingDocument15 pagesCattle RaisingJoey Dumaluan100% (1)
- Effect of Physiotherapy Rehabilitation On Volkmann Ischemic Contracture-A Case StudyDocument2 pagesEffect of Physiotherapy Rehabilitation On Volkmann Ischemic Contracture-A Case StudyIntan HaddadNo ratings yet
- DepakoteDocument5 pagesDepakotejNo ratings yet
- A Balanced Diet Is One That Provides An Adequate Intake of Energy and Nutrients For Maintenance of The Body and Therefore Good HealthDocument1 pageA Balanced Diet Is One That Provides An Adequate Intake of Energy and Nutrients For Maintenance of The Body and Therefore Good HealthSnigdha SarkarNo ratings yet
- Sandra Shroff Rofel College of NursingDocument27 pagesSandra Shroff Rofel College of NursingMehzbeen NavsariwalaNo ratings yet
- National Institute On Aging Publications CatalogDocument32 pagesNational Institute On Aging Publications CatalogAbex ComprasNo ratings yet
- Gabriel Ogun StateDocument15 pagesGabriel Ogun Statedavid ojNo ratings yet
- 2006 Surgery Final 6th YearDocument13 pages2006 Surgery Final 6th Yearmarina_shawkyNo ratings yet
- CDHO Factsheet Rheumatoid ArthritisDocument3 pagesCDHO Factsheet Rheumatoid ArthritisHenry MandalasNo ratings yet
- Herbal PlantsDocument14 pagesHerbal Plantsapi-3739910100% (2)
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- History of Psychosomatic Medicine BlumenfeldDocument20 pagesHistory of Psychosomatic Medicine Blumenfeldtatih meilaniNo ratings yet
- 1 MED Notes Diagnostic Criteria For SLEDocument4 pages1 MED Notes Diagnostic Criteria For SLEGustav G' GordonNo ratings yet
- Non-Plaque Induced GingivitisDocument30 pagesNon-Plaque Induced GingivitisDentist AymanNo ratings yet
- Dr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017Document45 pagesDr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017nanikNo ratings yet
- Journal ReadingDocument17 pagesJournal ReadingDesty Friska KurniaNo ratings yet
- 342 MCQDocument4 pages342 MCQRAJESH SHARMA100% (1)
- FengShui Inspection IDocument52 pagesFengShui Inspection IDavid Hu100% (3)