You might also like
- Ovarian CystDocument11 pagesOvarian CystVanessa Chavez DucayNo ratings yet
- Cholangitis Symptoms, Causes, Treatment GuideDocument15 pagesCholangitis Symptoms, Causes, Treatment GuideFaye TanNo ratings yet
- St. Paul University Quezon City College of Health Sciences case study on CholedocholithiasisDocument5 pagesSt. Paul University Quezon City College of Health Sciences case study on CholedocholithiasisJanelle Kate SaleNo ratings yet
- Acute Cholangitis - Background, Pathophysiology, EpidemiologyDocument3 pagesAcute Cholangitis - Background, Pathophysiology, Epidemiologym.m.m.mNo ratings yet
- Dermoid CystDocument29 pagesDermoid CystAlik ChuaNo ratings yet
- Gastrointestinal System Block: Case 4BDocument10 pagesGastrointestinal System Block: Case 4BRonald ChrisbiantoNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diaphragmatic Hernias: Symptoms, Types, and TreatmentDocument13 pagesDiaphragmatic Hernias: Symptoms, Types, and TreatmentOlga CerlatNo ratings yet
- Endometriosis: OccurrenceDocument6 pagesEndometriosis: Occurrencewea xczNo ratings yet
- Pathophysiology: Rectal CarcinomaDocument25 pagesPathophysiology: Rectal CarcinomaCristina CristinaNo ratings yet
- Mucinous Cystadenoma 0708Document12 pagesMucinous Cystadenoma 0708eosfieldNo ratings yet
- Laryngeal Cancer Causes, Symptoms, and TreatmentDocument36 pagesLaryngeal Cancer Causes, Symptoms, and TreatmentJayson de GuzmanNo ratings yet
- Nursing Process OsteosarcomaDocument34 pagesNursing Process OsteosarcomaDonJohnNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Rectal CarcinomaDocument16 pagesRectal Carcinomabuddy557No ratings yet
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- Nomad: Physiology of PregnancyDocument28 pagesNomad: Physiology of PregnancyDr.M.Anthony David83% (6)
- Small Bowel ObstructionDocument2 pagesSmall Bowel ObstructionSrividya PushpalaNo ratings yet
- Cholelithiasis 0232Document118 pagesCholelithiasis 0232Kz LonerNo ratings yet
- PATHOPHYSIOLOGY of NeurocysticercosisDocument6 pagesPATHOPHYSIOLOGY of Neurocysticercosisteddydeclines14100% (3)
- Hysterectomy and Bilateral Salpingo-OophorectomyDocument1 pageHysterectomy and Bilateral Salpingo-Oophorectomyapi-3712326100% (3)
- Clinical Scenario and Worksheet For Diagnostic Appraisal (Journal On Dengue)Document3 pagesClinical Scenario and Worksheet For Diagnostic Appraisal (Journal On Dengue)Stephie E.No ratings yet
- Obstetrics Midterms Rationale 2nd Sem 2018 2019Document21 pagesObstetrics Midterms Rationale 2nd Sem 2018 2019Gene Paulo UyNo ratings yet
- 1 LiverDocument10 pages1 LiverAlbino Fulgencio Santos III100% (1)
- Robotic SurgeryDocument10 pagesRobotic Surgerys_asmathNo ratings yet
- Case Study #5Document2 pagesCase Study #5Jenny Jenders100% (1)
- Testicular CancerDocument24 pagesTesticular CancerJulianne LeeNo ratings yet
- Case Study Acute Lymphoid LeukemiaDocument1 pageCase Study Acute Lymphoid Leukemia2literNo ratings yet
- Acute Lymphocytic LeukemiaDocument7 pagesAcute Lymphocytic Leukemiamildred alidon100% (1)
- Laryngeal CancerDocument3 pagesLaryngeal Cancerneilclaudio0% (1)
- Diagnosis of Portal Hypertension 1Document20 pagesDiagnosis of Portal Hypertension 1sussie jeffersonNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- Evaluation of Abdominal PainDocument7 pagesEvaluation of Abdominal PainCherry Faith Merisco LabtangNo ratings yet
- Case 2 and 3 Q1Document3 pagesCase 2 and 3 Q1Jeffrey Ramos0% (1)
- Acromegaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcromegaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Surgical Review On HypospadiasDocument30 pagesSurgical Review On Hypospadiasbakukangtribe100% (1)
- New Concepts in the Management of Septic Perianal ConditionsFrom EverandNew Concepts in the Management of Septic Perianal ConditionsNo ratings yet
- Case Presentation-ChickenpoxDocument41 pagesCase Presentation-ChickenpoxShaliniNo ratings yet
- Clinical Practice Guidelines: Chronic Suppurative Otitis Media in AdultsDocument28 pagesClinical Practice Guidelines: Chronic Suppurative Otitis Media in Adultsnanu-jenuNo ratings yet
- Pancreatic AdenocarcinomaDocument6 pagesPancreatic AdenocarcinomafikriafisNo ratings yet
- A Giant Juvenile Fibroadenoma of BreastDocument2 pagesA Giant Juvenile Fibroadenoma of BreastIOSRjournalNo ratings yet
- Gastric CancerDocument7 pagesGastric CancerMicah PingawanNo ratings yet
- Preeclampsia UpToDateDocument60 pagesPreeclampsia UpToDateMauricio Marin MontoyaNo ratings yet
- Testicular CancerDocument48 pagesTesticular Cancerluckyswiss7776848No ratings yet
- Video-Assisted Thoracoscopic Surgery (Vats) in ChildrenDocument24 pagesVideo-Assisted Thoracoscopic Surgery (Vats) in ChildrenobrankovNo ratings yet
- MSU Buug College Nursing Assessment for Abdominal PainDocument30 pagesMSU Buug College Nursing Assessment for Abdominal Painllanelli.graciaNo ratings yet
- Cancer of The LarynxDocument16 pagesCancer of The Larynxhelaley_1983No ratings yet
- Upper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Document10 pagesUpper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Angelo Dela Cruz VillaromanNo ratings yet
- Cholelithiasis Treatment & ManagementDocument8 pagesCholelithiasis Treatment & ManagementRayhanun MardhatillahNo ratings yet
- Gastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDocument31 pagesGastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDeep KhemaniNo ratings yet
- Renal Concept MapDocument8 pagesRenal Concept MapXtine CajiNo ratings yet
- 2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFDocument4 pages2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFteteh_thikeuNo ratings yet
- Gallstone Case StudyDocument19 pagesGallstone Case StudyMoNa JbaReenNo ratings yet
- Pathology Polycystic Kidney DiseaseDocument4 pagesPathology Polycystic Kidney DiseaseOnyedika EgbujoNo ratings yet
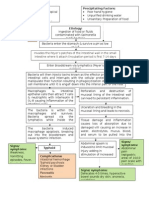
- Pathophysiology of CholangitisDocument4 pagesPathophysiology of CholangitisAmni 'Pam' Zulkifar100% (1)
- Nodular Goiter Concept MapDocument5 pagesNodular Goiter Concept MapAllene PaderangaNo ratings yet
- Intestinal ObstructionDocument48 pagesIntestinal ObstructionMahmoud AbuAwadNo ratings yet
- Intussusception PresentationDocument9 pagesIntussusception PresentationAme NasokiaNo ratings yet
- Septic ArthritisDocument6 pagesSeptic ArthritisIfit Bagus ApriantonoNo ratings yet
- CAP Flow Sheet PDF 62015 PDFDocument1 pageCAP Flow Sheet PDF 62015 PDFroshmaeNo ratings yet
- SHEDocument3 pagesSHEroshmaeNo ratings yet
- Coagulation Cascade: Difference Between Intrinsic and Extrinsic PathwayDocument10 pagesCoagulation Cascade: Difference Between Intrinsic and Extrinsic Pathwayroshmae100% (1)
- Cap PDFDocument1 pageCap PDFroshmaeNo ratings yet
- Gyne - Congenital HypothyroidismDocument3 pagesGyne - Congenital HypothyroidismroshmaeNo ratings yet
- IM - Focal Seizure ReportDocument2 pagesIM - Focal Seizure ReportroshmaeNo ratings yet
- Surgery - PAODDocument4 pagesSurgery - PAODroshmaeNo ratings yet
- CPG Pcap 2012 PDFDocument54 pagesCPG Pcap 2012 PDFroshmae67% (3)
- CAP Flow Sheet PDF 62015 PDFDocument1 pageCAP Flow Sheet PDF 62015 PDFroshmaeNo ratings yet
- Sentinel Lymph Node DissectionDocument9 pagesSentinel Lymph Node DissectionroshmaeNo ratings yet
- FCM IiiDocument2 pagesFCM IiiroshmaeNo ratings yet
- Causes and Symptoms of HypothyroidismDocument3 pagesCauses and Symptoms of HypothyroidismroshmaeNo ratings yet
- IM - Focal Seizure ReportDocument8 pagesIM - Focal Seizure ReportroshmaeNo ratings yet
- PD Surgery - Incarcerated Hernia - Dr. RanaDocument2 pagesPD Surgery - Incarcerated Hernia - Dr. RanaroshmaeNo ratings yet
- BP: HR: RR: Temp:: CBC Count Pulse Oximetry (Oxygen Saturation) CreatinineDocument2 pagesBP: HR: RR: Temp:: CBC Count Pulse Oximetry (Oxygen Saturation) CreatinineroshmaeNo ratings yet
- Topic:: Obejctives Content TA T-L Activitie S Materials Resources Evaluatio NDocument2 pagesTopic:: Obejctives Content TA T-L Activitie S Materials Resources Evaluatio NroshmaeNo ratings yet
- PD - Heart Failure ReportDocument28 pagesPD - Heart Failure ReportroshmaeNo ratings yet
- POT - NutritionDocument18 pagesPOT - NutritionroshmaeNo ratings yet
- Surgery 1Document2 pagesSurgery 1roshmaeNo ratings yet
- PD - CopdDocument3 pagesPD - CopdroshmaeNo ratings yet
- Recommendations 1Document1 pageRecommendations 1roshmaeNo ratings yet
- ResearchDocument3 pagesResearchroshmaeNo ratings yet
- ACS WorksheetDocument6 pagesACS WorksheetroshmaeNo ratings yet
- Cervical CancerDocument32 pagesCervical CancervvmgkikiNo ratings yet
- Gyne - Functional Ovarian Cysts Treatment and ManagementDocument1 pageGyne - Functional Ovarian Cysts Treatment and ManagementroshmaeNo ratings yet
- ACS WorksheetDocument6 pagesACS WorksheetroshmaeNo ratings yet
- After Bea's PPT Psych Reports. 4.5 - 4.6Document51 pagesAfter Bea's PPT Psych Reports. 4.5 - 4.6roshmaeNo ratings yet
- PD - Heart Failure ReportDocument28 pagesPD - Heart Failure ReportroshmaeNo ratings yet
- Typhoid Fever PathophysiologyDocument1 pageTyphoid Fever PathophysiologyroshmaeNo ratings yet
- Case 1 Gyne ID, PEDocument2 pagesCase 1 Gyne ID, PEroshmaeNo ratings yet
- The Ultimate BLS CheatsheetDocument30 pagesThe Ultimate BLS CheatsheetAimee Eichler100% (2)
- Macrocytic Anemia - Megaloblastic AnemiaDocument42 pagesMacrocytic Anemia - Megaloblastic AnemiaDarien LiewNo ratings yet
- The Value of Urine Specific Gravity in Detecting Diabetes Insipidus in A Patient With DMDocument2 pagesThe Value of Urine Specific Gravity in Detecting Diabetes Insipidus in A Patient With DMFaryalBalochNo ratings yet
- Alopecia Areata in Covid 19 Case ReportDocument2 pagesAlopecia Areata in Covid 19 Case ReportAnti TjahyaNo ratings yet
- Nosocomial Infection?Document4 pagesNosocomial Infection?Sara ANo ratings yet
- Critical care guidelines for IV nicardipine useDocument3 pagesCritical care guidelines for IV nicardipine useLisa Trisnawati ChaniagoNo ratings yet
- MedicineDocument49 pagesMedicinesnagltNo ratings yet
- DISCHARGE INSTRUCTIONSDocument7 pagesDISCHARGE INSTRUCTIONSJyselle Domingo100% (4)
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapybgfhnfgNo ratings yet
- Web KFOG-jan-11Document16 pagesWeb KFOG-jan-11kutra3000No ratings yet
- Toxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDDocument8 pagesToxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDGoran TomićNo ratings yet
- Placental Abnormalities: Placenta Accreta, Placenta Increta, and Placenta PercretaDocument11 pagesPlacental Abnormalities: Placenta Accreta, Placenta Increta, and Placenta PercretaLiza M. PurocNo ratings yet
- Trichuris TrichiuraDocument3 pagesTrichuris TrichiuraTwish BeraldeNo ratings yet
- ITLS 8e Advanced Post Test Exam Version BDocument10 pagesITLS 8e Advanced Post Test Exam Version BMohamed TabanaNo ratings yet
- Keeping Abreast of Future Need - A Report Into The Growing Demand For Breast Care NursesDocument14 pagesKeeping Abreast of Future Need - A Report Into The Growing Demand For Breast Care NursesEmmaNo ratings yet
- Rice DiseaseDocument23 pagesRice DiseaseRayge HarbskyNo ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- Designated Medical Event Dme List enDocument3 pagesDesignated Medical Event Dme List enAmany HagageNo ratings yet
- Cerebral PalsyDocument11 pagesCerebral PalsyLawrence BellNo ratings yet
- Herpes Simplex I and IIDocument50 pagesHerpes Simplex I and IItummalapalli venkateswara raoNo ratings yet
- ECSI Instructor Update 2021Document52 pagesECSI Instructor Update 2021Zach MatthewsNo ratings yet
- Hesi Med Surg-14Document1 pageHesi Med Surg-14GeorgeNo ratings yet
- 127 FullDocument9 pages127 FullCho HyumiNo ratings yet
- Umbilical Vein CatheterizationDocument3 pagesUmbilical Vein CatheterizationrohitNo ratings yet
- Indriatmi, W. 2018. Ilmu Penyakit Dan Kulit Kelamin. Edisi Ke-7. Jakarta: Badan Penerbit Fakultas Kedokteran IndonesiaDocument10 pagesIndriatmi, W. 2018. Ilmu Penyakit Dan Kulit Kelamin. Edisi Ke-7. Jakarta: Badan Penerbit Fakultas Kedokteran IndonesiaDiza Hanni PertiwiNo ratings yet
- Non-ST Elevation Myocardial Infarction (NSTEMI) Case ReportDocument28 pagesNon-ST Elevation Myocardial Infarction (NSTEMI) Case ReportuculucullNo ratings yet
- Nursing Diagnoses and Planning Across the LifespanDocument64 pagesNursing Diagnoses and Planning Across the LifespanßläcklìsètèdTȜèNo ratings yet
- Coronary Artery Disease (CAD) Angina Pectoris: Chapter 28: Management of Patients With CVDDocument3 pagesCoronary Artery Disease (CAD) Angina Pectoris: Chapter 28: Management of Patients With CVDLizzy WayNo ratings yet
- Cardiac Marker Sem 5Document42 pagesCardiac Marker Sem 5novi pujiNo ratings yet
- Overview HyperparatiroidDocument5 pagesOverview HyperparatiroiddyahNo ratings yet