You might also like
- Guidelines for Diagnosing and Managing Delirium in the ElderlyDocument22 pagesGuidelines for Diagnosing and Managing Delirium in the ElderlyMutia OktaviaNo ratings yet
- Guidelines for Diagnosing and Managing Delirium in the ElderlyDocument22 pagesGuidelines for Diagnosing and Managing Delirium in the ElderlyMutia OktaviaNo ratings yet
- OutputDocument27 pagesOutputMutia OktaviaNo ratings yet
- OutputDocument27 pagesOutputMutia OktaviaNo ratings yet
- OutputDocument27 pagesOutputMutia OktaviaNo ratings yet
- OutputDocument27 pagesOutputMutia OktaviaNo ratings yet
- OutputDocument27 pagesOutputMutia OktaviaNo ratings yet
- OutputDocument27 pagesOutputMutia OktaviaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Intravenous Cannulation IV OSCE GuideDocument11 pagesIntravenous Cannulation IV OSCE GuideBasmah 7No ratings yet
- Soal No.1 Bedah DigestifDocument11 pagesSoal No.1 Bedah DigestifRaniPradnyaSwariNo ratings yet
- Shoulder Concepts 2013: Consensus and ConcernsDocument99 pagesShoulder Concepts 2013: Consensus and ConcernsMichel HovsepianNo ratings yet
- Gore EndoprotesesDocument4 pagesGore EndoprotesesLivio NakanoNo ratings yet
- Hiatal Hernia: BY MR, Vinay KumarDocument27 pagesHiatal Hernia: BY MR, Vinay KumarVinay KumarNo ratings yet
- ACL Reconstruction With The ACUFEX™ Director Drill Guide and Endobutton™ CL Fixation SystemDocument12 pagesACL Reconstruction With The ACUFEX™ Director Drill Guide and Endobutton™ CL Fixation Systemapi-19808945No ratings yet
- NeonatalresuscitationDocument67 pagesNeonatalresuscitationfidaNo ratings yet
- ACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL DaDocument209 pagesACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL Dajelena_stankovic_34No ratings yet
- Brochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Document12 pagesBrochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Andreea L. MihalceaNo ratings yet
- Flabby RidgeDocument7 pagesFlabby RidgeRaksmey PhanNo ratings yet
- Mock Exam - Key AnswersDocument8 pagesMock Exam - Key Answerscrsdzx4c9gNo ratings yet
- AARC Clinical Practice GuidelineDocument23 pagesAARC Clinical Practice GuidelineModsom OouiNo ratings yet
- Transportation of The Critically Ill Patient 1Document17 pagesTransportation of The Critically Ill Patient 1Foo Wing JianNo ratings yet
- The Marketing Mix of Apollo Hospitals Discusses The Service Marketing Mix or The 7PDocument12 pagesThe Marketing Mix of Apollo Hospitals Discusses The Service Marketing Mix or The 7Pwaseem100% (1)
- Mcqs On Excretory SystemDocument3 pagesMcqs On Excretory SystemIshfaq LoneNo ratings yet
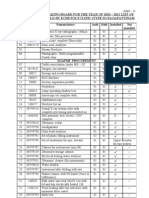
- Annual Stock Taking Board For The Year of 2010 - 2011 List of Maj Med Eqpt-Held by Echs Polyclinic (Type-D) NagapattinamDocument17 pagesAnnual Stock Taking Board For The Year of 2010 - 2011 List of Maj Med Eqpt-Held by Echs Polyclinic (Type-D) NagapattinamechsngtNo ratings yet
- Human Skeletal System PPTDocument73 pagesHuman Skeletal System PPTInsatiable CleeNo ratings yet
- 14Document18 pages14JuliusNo ratings yet
- Surgical and Anaesthetic Instruments For OSCEs - A Practical Study Guide (Master Pass Series) 1st EditionDocument121 pagesSurgical and Anaesthetic Instruments For OSCEs - A Practical Study Guide (Master Pass Series) 1st EditionYoleima PerdomoNo ratings yet
- Transoral Laser MicrosurgeryDocument4 pagesTransoral Laser MicrosurgeryanniebuhrNo ratings yet
- Kepaniteraan Klinik Senior Bagian Ilmu Bedah OrthopaedicDocument19 pagesKepaniteraan Klinik Senior Bagian Ilmu Bedah OrthopaedicPutraNo ratings yet
- Clinical Success in Surgical and Orthodontic Treatment of Impacted Teeth - Jean-Marie KORBENDAU, Antomio PATTI 2006Document251 pagesClinical Success in Surgical and Orthodontic Treatment of Impacted Teeth - Jean-Marie KORBENDAU, Antomio PATTI 2006anh le ducNo ratings yet
- Osteocel Plus BrochureDocument2 pagesOsteocel Plus Brochureapi-235072265No ratings yet
- Meniscus Tears - Cartilage Damage: KneeDocument9 pagesMeniscus Tears - Cartilage Damage: KneedheenadayalanNo ratings yet
- CORDOCENTESISDocument6 pagesCORDOCENTESISSagar HanamasagarNo ratings yet
- SEO-Optimized Title for Spinal Pain DocumentDocument37 pagesSEO-Optimized Title for Spinal Pain Documentsiddharthnair_1100% (1)
- Prophecy Neuro ICU Exam Content OutlineDocument5 pagesProphecy Neuro ICU Exam Content OutlineDarren DawkinsNo ratings yet
- Curaplex-EMP Defib Pads Ref Chart 01 19Document1 pageCuraplex-EMP Defib Pads Ref Chart 01 19Vikki LeonardiNo ratings yet
- Teeth in a Day: The Branemark Novum SystemDocument4 pagesTeeth in a Day: The Branemark Novum SystemSatyendra KumarNo ratings yet
- (Cundiff, Geoffrey W. Te Linde, Richard Wesley) T (B-Ok - Xyz) PDFDocument382 pages(Cundiff, Geoffrey W. Te Linde, Richard Wesley) T (B-Ok - Xyz) PDFAna Adam80% (5)