You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Bitcoin WhoDocument6 pagesBitcoin WhoPeiter FitzpatrickNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Bitcoin WhoDocument6 pagesBitcoin WhoPeiter FitzpatrickNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Bitcoin WhoDocument6 pagesBitcoin WhoPeiter FitzpatrickNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- How Did Our Immune System Become So ComplexDocument2 pagesHow Did Our Immune System Become So ComplexpopophobiaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- NASA/TM-2002-211716 An Introduction To Tensors For Students of Physics and Engineering Joseph C. Kolecki Glenn Research Center, Cleveland, OhioDocument29 pagesNASA/TM-2002-211716 An Introduction To Tensors For Students of Physics and Engineering Joseph C. Kolecki Glenn Research Center, Cleveland, OhiomarkrichardmuradNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- KINESIOLOGY CHAPTER 2 MOVEMENTSDocument36 pagesKINESIOLOGY CHAPTER 2 MOVEMENTSZuhaib AhmedNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Learning Episode 1 Educational Theories - PONIENTEDocument10 pagesLearning Episode 1 Educational Theories - PONIENTECid Poniente100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Presentation by Prof Katya Rubia - The Change Within: Sustainable Effects Ofsustainable Effects of Meditation On Healthmeditation On HealthDocument24 pagesPresentation by Prof Katya Rubia - The Change Within: Sustainable Effects Ofsustainable Effects of Meditation On Healthmeditation On Healthtanaha100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Effects of Jealousy in A RelationshipDocument2 pagesEffects of Jealousy in A RelationshipShyla Bantolinao100% (1)
- Come Back To Your Senses Use Your Body: Psychologyt LsDocument1 pageCome Back To Your Senses Use Your Body: Psychologyt LsMarina Moran100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Jack FullerDocument9 pagesJack FullerLAURA OLIVOSNo ratings yet
- Dahraan Mental Hospital Marka Mental Health CareDocument8 pagesDahraan Mental Hospital Marka Mental Health CareJossephNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Can Animals Understand Human LanguageDocument2 pagesCan Animals Understand Human LanguageLada BurlakaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Nature Vs NurtureDocument7 pagesNature Vs NurtureDeepaPandeyNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Trauma and Self CareDocument54 pagesTrauma and Self CarerimshaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Learning Neural Activations: Fayyaz Ul Amir Afsar Minhas and Amina AsifDocument10 pagesLearning Neural Activations: Fayyaz Ul Amir Afsar Minhas and Amina AsifssrefrNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Break Free - Nathaniel BrandenDocument16 pagesBreak Free - Nathaniel Brandennbckudxtkudkuf50% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Lesson Plan - CotDocument8 pagesLesson Plan - CotRutchie Quillo TuandoNo ratings yet
- Philippians 4 13 - PPT DEFENSEDocument17 pagesPhilippians 4 13 - PPT DEFENSESherwina Marie del RosarioNo ratings yet
- Ursula E. Oberst, Alan E. Stewart - Adlerian Psych PDFDocument235 pagesUrsula E. Oberst, Alan E. Stewart - Adlerian Psych PDFRadu PrusanNo ratings yet
- CT I MRI Tumora MozgaDocument126 pagesCT I MRI Tumora MozgaElvir MalicevicNo ratings yet
- Guidance Approach For The Encouraging Classroom 6th Edition Dan Gartrell Test BankDocument3 pagesGuidance Approach For The Encouraging Classroom 6th Edition Dan Gartrell Test Banka878027987No ratings yet
- Hiperakusis 2015Document20 pagesHiperakusis 2015Abdur ShamilNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Theories of Human Motivation in An Organization: Audrey Therese C. Fulgencio and Jessa D. AnasDocument32 pagesTheories of Human Motivation in An Organization: Audrey Therese C. Fulgencio and Jessa D. AnasJessamae AnasNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanJustine Suico100% (1)
- MotivationDocument9 pagesMotivationarsal169100% (1)
- Theories of Learning and Learning MetaphorsDocument4 pagesTheories of Learning and Learning MetaphorsTrisha Mei Nagal50% (2)
- DLL - English 2 - Q1 - W1Document4 pagesDLL - English 2 - Q1 - W1Carino ArleneNo ratings yet
- Alzheimer Disease - Risks, Symptoms and Related TestsDocument15 pagesAlzheimer Disease - Risks, Symptoms and Related TestsMishelaNo ratings yet
- Week 8 Assignment (Perception)Document2 pagesWeek 8 Assignment (Perception)JASFEEQREE BIN JASMIH -No ratings yet
- Soft Skills Guiding NotesDocument34 pagesSoft Skills Guiding NotesRajick MusiqNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Traumata and ConsequencesFr RuppertDocument36 pagesTraumata and ConsequencesFr Ruppertrodicachirculescu100% (1)
- Saladaga, Kean Debert T.: ReviewsDocument4 pagesSaladaga, Kean Debert T.: ReviewsKean Debert SaladagaNo ratings yet
- Music Psychology in Education Bedford Way Papers Book 25Document289 pagesMusic Psychology in Education Bedford Way Papers Book 25Xavier Cevallos100% (1)
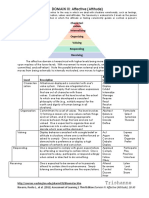
- Trishanne: DOMAIN III: Affective (Attitude)Document2 pagesTrishanne: DOMAIN III: Affective (Attitude)ᜆ᜔ᜇᜒᜐ᜔ᜑ᜔ ᜀᜈ᜔No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)