You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Check - Unit - 554 - October - Renal - Problems V2 PDFDocument26 pagesCheck - Unit - 554 - October - Renal - Problems V2 PDFdragon660% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pearson - Vue - 200 QUESTIONS PDFDocument40 pagesPearson - Vue - 200 QUESTIONS PDFDr-Jahanzaib Gondal100% (2)
- Annex A - Driver's Medical Evaluation Form (August 8 2018) - 2Document2 pagesAnnex A - Driver's Medical Evaluation Form (August 8 2018) - 2Dhon de CastroNo ratings yet
- DiaDENS-PC Operation ManualDocument72 pagesDiaDENS-PC Operation Manualgetdenas100% (7)
- Malaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaDocument27 pagesMalaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaAnonymous Di1zSIkRBHNo ratings yet
- Classification of Congenital Heart DiseaseDocument1 pageClassification of Congenital Heart DiseaseAnonymous Di1zSIkRBHNo ratings yet
- Sepsis Update 2017 - 2Document49 pagesSepsis Update 2017 - 2Ahmad Fathul Adzmi100% (1)
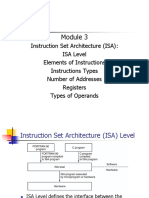
- Instruction Set Architecture (ISA) : ISA Level Elements of Instructions Instructions Types Number of Addresses Registers Types of OperandsDocument51 pagesInstruction Set Architecture (ISA) : ISA Level Elements of Instructions Instructions Types Number of Addresses Registers Types of OperandsAnonymous Di1zSIkRBHNo ratings yet
- Who 2014Document100 pagesWho 2014Anonymous Di1zSIkRBHNo ratings yet
- Report of Treasurer RusDocument5 pagesReport of Treasurer RusAnonymous Di1zSIkRBHNo ratings yet
- 54 5 5 PDFDocument7 pages54 5 5 PDFTri Umi Maslakhatut DiniahNo ratings yet
- Presentasi Modul 1Document16 pagesPresentasi Modul 1Anonymous Di1zSIkRBHNo ratings yet
- PLENO21CKULITDocument20 pagesPLENO21CKULITAnonymous Di1zSIkRBHNo ratings yet
- After Studying This ChapterDocument2 pagesAfter Studying This ChapterAnonymous Di1zSIkRBHNo ratings yet
- CoolmanDocument7 pagesCoolmanAnonymous Di1zSIkRBHNo ratings yet
- Implikasi Bla2Document7 pagesImplikasi Bla2Anonymous Di1zSIkRBHNo ratings yet
- Hepatoprotective Constituents of Firmiana Hepatocytes WebsiteDocument2 pagesHepatoprotective Constituents of Firmiana Hepatocytes WebsiteAnonymous Di1zSIkRBHNo ratings yet
- PlenoDocument17 pagesPlenoAnonymous Di1zSIkRBHNo ratings yet
- Pleno PresentationDocument14 pagesPleno PresentationAnonymous Di1zSIkRBHNo ratings yet
- Hepatoprotective Constituents of Firmiana Hepatocytes WebsiteDocument2 pagesHepatoprotective Constituents of Firmiana Hepatocytes WebsiteAnonymous Di1zSIkRBHNo ratings yet
- Presentation 1Document2 pagesPresentation 1Anonymous Di1zSIkRBHNo ratings yet
- Presentation 2Document2 pagesPresentation 2Anonymous Di1zSIkRBHNo ratings yet
- Kuliah OiDocument61 pagesKuliah OiNovasuryatiNo ratings yet
- JadwalDocument1 pageJadwalAnonymous Di1zSIkRBHNo ratings yet
- Pathogenesis of AtherosclerosisDocument1 pagePathogenesis of AtherosclerosisAnonymous Di1zSIkRBHNo ratings yet
- Slide Progosis Dan KomplikasDocument2 pagesSlide Progosis Dan KomplikasAnonymous Di1zSIkRBHNo ratings yet
- Third Party Legal NoticesDocument1 pageThird Party Legal NoticesvincexianNo ratings yet
- SkemaDocument1 pageSkemaAnonymous Di1zSIkRBHNo ratings yet
- GetAmped2ClientSoftwareLicenseAgreement HKDocument2 pagesGetAmped2ClientSoftwareLicenseAgreement HKAnonymous Di1zSIkRBHNo ratings yet
- InfeksiDocument2 pagesInfeksiAnonymous Di1zSIkRBHNo ratings yet
- Inflation ExpectationsasaDocument29 pagesInflation ExpectationsasaAnonymous Di1zSIkRBHNo ratings yet
- F4 SC Nota Bab 3 Techniques of Measuring The Parameters of Body HealthDocument13 pagesF4 SC Nota Bab 3 Techniques of Measuring The Parameters of Body HealthJIanyun ChanNo ratings yet
- Case Study: Treating Hypertension in Patients With DiabetesDocument10 pagesCase Study: Treating Hypertension in Patients With Diabetesfirda rydNo ratings yet
- Community Health Survey ToolDocument6 pagesCommunity Health Survey ToolYna EstabilloNo ratings yet
- 312 Lec Cu10Document4 pages312 Lec Cu10Carl SantosNo ratings yet
- Sab Theek ReportDocument8 pagesSab Theek ReportAyusmanNo ratings yet
- Diagnosis of Pulmonary HypertensionDocument12 pagesDiagnosis of Pulmonary HypertensionFaridaFaradillaPutryCherewetNo ratings yet
- Health Problem Family Nursing Problem Goal of Care Objectives of Care Intervention PlanDocument2 pagesHealth Problem Family Nursing Problem Goal of Care Objectives of Care Intervention PlanCarol MalcoNo ratings yet
- Operative Orthopaedics Stanmore Guide 2010Document329 pagesOperative Orthopaedics Stanmore Guide 2010Shourjendra Datta100% (11)
- Ehx 273Document4 pagesEhx 273Robby Paguh TariganNo ratings yet
- Pre Eclampsia Eclampsia Guideline For The Management of SevereDocument15 pagesPre Eclampsia Eclampsia Guideline For The Management of SevereAris SaptianNo ratings yet
- Discussion: Cardiovascular Disease Mini-Case Study Case Study #2 Cardiovascular DiseaseDocument3 pagesDiscussion: Cardiovascular Disease Mini-Case Study Case Study #2 Cardiovascular Diseaseapi-546898544No ratings yet
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDocument7 pagesIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaNo ratings yet
- Acute Ischemic Stroke: Clinical PracticeDocument8 pagesAcute Ischemic Stroke: Clinical PracticeDorina FrunzeNo ratings yet
- Nur 111 Session 15 Sas 1Document8 pagesNur 111 Session 15 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Unit 8 BSC 3rd YearDocument20 pagesUnit 8 BSC 3rd Yearsimonjosan100% (2)
- Afif Zikri Bin Abd Aziz - Eh2204wwDocument8 pagesAfif Zikri Bin Abd Aziz - Eh2204wwMOHD MU'IZZ MOHD SHUKRINo ratings yet
- Case Study HypertensionDocument29 pagesCase Study HypertensionnilamNo ratings yet
- Angel Hill's ThesisDocument45 pagesAngel Hill's ThesisJoan MelendresNo ratings yet
- 21 TranslatedDocument71 pages21 TranslatedMerry MonroeNo ratings yet
- Stroke in Pregnancy and The Puerperium: S D Treadwell, B Thanvi, T G RobinsonDocument8 pagesStroke in Pregnancy and The Puerperium: S D Treadwell, B Thanvi, T G RobinsonNabillah MukhlisNo ratings yet
- 12 Physical Education English Medium Chapter PDFDocument36 pages12 Physical Education English Medium Chapter PDFRohit0% (1)
- Medical Examination Report: A. Examinee DetailsDocument4 pagesMedical Examination Report: A. Examinee DetailsMohammed Bilal ShaikNo ratings yet
- NTRN 516 Case Study 2 - DM 10 12 15 UpdateDocument18 pagesNTRN 516 Case Study 2 - DM 10 12 15 Updateapi-315324296No ratings yet
- MAPEH 9 Second GradingDocument9 pagesMAPEH 9 Second GradingSittie Rahma AlawiNo ratings yet
- MidtermDocument53 pagesMidtermwriter topNo ratings yet
- 2022 05 CK May GK Shots PDFDocument262 pages2022 05 CK May GK Shots PDFCommon PhoneNo ratings yet