You might also like
- Are Women With Recurrent Spontaneous Preterm Births Different From Those Without Such HistoryDocument9 pagesAre Women With Recurrent Spontaneous Preterm Births Different From Those Without Such HistoryMichael HusainNo ratings yet
- Natural History of Fetal Position During Pregnancy.11Document6 pagesNatural History of Fetal Position During Pregnancy.11PutriNo ratings yet
- Zhang 2019Document9 pagesZhang 2019Maria José MendiolaNo ratings yet
- Can Placental Growth Factor in Maternal Circulation Identify Fetuses With Placental Intrauterine Growth RestrictionDocument7 pagesCan Placental Growth Factor in Maternal Circulation Identify Fetuses With Placental Intrauterine Growth RestrictionagusNo ratings yet
- WoMPBI9 Abstracts PDFDocument101 pagesWoMPBI9 Abstracts PDFMartha EndikaNo ratings yet
- $116 SMFM AbstractsDocument1 page$116 SMFM AbstractsSheila Regina TizaNo ratings yet
- Articulos Sepsis Neonatal TempranaDocument29 pagesArticulos Sepsis Neonatal Tempranaverock88No ratings yet
- Asymptomatic Bacterial Vaginosis and Intermediate Flora As Risk Factors For Adverse Pregnancy OutcomeDocument16 pagesAsymptomatic Bacterial Vaginosis and Intermediate Flora As Risk Factors For Adverse Pregnancy OutcomealvilNo ratings yet
- Senapati2018 Article SuperovulationAltersTheExpressDocument10 pagesSenapati2018 Article SuperovulationAltersTheExpressInneke NoerNo ratings yet
- HHS Public AccessDocument25 pagesHHS Public AccessIdmNo ratings yet
- Placenta Accreta Is Associated With IVF Pregnancies: A Retrospective Chart ReviewDocument6 pagesPlacenta Accreta Is Associated With IVF Pregnancies: A Retrospective Chart ReviewGladstone AsadNo ratings yet
- Jurnal OG 4Document11 pagesJurnal OG 4Reka AmeliaNo ratings yet
- Leitich, 2003 Antibiotico No Tratamento de VB Meta AnaliseDocument7 pagesLeitich, 2003 Antibiotico No Tratamento de VB Meta AnaliseEdgar SimmonsNo ratings yet
- Predictive value of maternal s erum β-hCG concentration in the ruptured tubal ectopic pregnancyDocument7 pagesPredictive value of maternal s erum β-hCG concentration in the ruptured tubal ectopic pregnancyyayayaNo ratings yet
- Wolf Et Al MultivitaminsDocument30 pagesWolf Et Al MultivitaminsAnonymous 2GBzrE3XNo ratings yet
- Awwad Et Al-2015-BJOG An International Journal of Obstetrics & GynaecologyDocument9 pagesAwwad Et Al-2015-BJOG An International Journal of Obstetrics & GynaecologyHervi LaksariNo ratings yet
- Jurnal KedokteranDocument6 pagesJurnal Kedokteranusk.ppdsobgynganjil2022No ratings yet
- Paper Cervical LenghtDocument30 pagesPaper Cervical LenghtDanTe D' WinchesterNo ratings yet
- Acta PaediatricaDocument13 pagesActa PaediatricaDefranky TheodorusNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- 57 Andrews2003 PDFDocument9 pages57 Andrews2003 PDFangela_karenina_1No ratings yet
- Preterm Parturition and Pre-Eclampsia: The Confluence of Two Great Gestational SyndromesDocument7 pagesPreterm Parturition and Pre-Eclampsia: The Confluence of Two Great Gestational SyndromesmarinanananaNo ratings yet
- 57 Andrews2003 PDFDocument9 pages57 Andrews2003 PDFangela_karenina_1No ratings yet
- 18-American Journal of Reproductive Immunology 2019 SistiDocument5 pages18-American Journal of Reproductive Immunology 2019 SistiSara PaccosiNo ratings yet
- Journal Pre-Proof: American Journal of Obstetrics and GynecologyDocument36 pagesJournal Pre-Proof: American Journal of Obstetrics and GynecologyLuis Martinez NavarroNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptJes LopNo ratings yet
- Spontaneous Preterm Birth Prevention in Multiple PregnancyDocument7 pagesSpontaneous Preterm Birth Prevention in Multiple PregnancyElias Melo JrNo ratings yet
- Morfologi PlasentaDocument6 pagesMorfologi PlasentayueldiNo ratings yet
- Accuracy of Cervico Vaginal Fetal Fibronectin Test in Predicting Risk of Spontaneous Preterm BirthDocument6 pagesAccuracy of Cervico Vaginal Fetal Fibronectin Test in Predicting Risk of Spontaneous Preterm BirthOpenaccess Research paperNo ratings yet
- 17-OHPC To Prevent Recurrent Preterm Birth in Singleton Gestations (PROLONG Study) : A Multicenter, International, Randomized Double-Blind TrialDocument10 pages17-OHPC To Prevent Recurrent Preterm Birth in Singleton Gestations (PROLONG Study) : A Multicenter, International, Randomized Double-Blind Trialomarmeftah838No ratings yet
- Gut Microbiota Signatures in Gestational AnemiaDocument9 pagesGut Microbiota Signatures in Gestational AnemiaTanushree PanjariNo ratings yet
- Original Article The Association of Bacterial Vaginosis and Preterm LaborDocument3 pagesOriginal Article The Association of Bacterial Vaginosis and Preterm LaborHarry ManuhutuNo ratings yet
- Increasing Fetal Ovine Number Per Gestation Alters Fetal Plasma Clinical Chemistry ValuesDocument12 pagesIncreasing Fetal Ovine Number Per Gestation Alters Fetal Plasma Clinical Chemistry ValuesHuang GlivecNo ratings yet
- 6 PGS缩短受孕时间Document8 pages6 PGS缩短受孕时间zjuwindNo ratings yet
- Morbidly Adherent Placenta Treatments and OutcomesDocument15 pagesMorbidly Adherent Placenta Treatments and OutcomesDara Mayang SariNo ratings yet
- Prediction of Preeclampsia Throughout Gestation With Maternal Characteristics and Biophysical and Biochemical Markers: A Longitudinal StudyDocument22 pagesPrediction of Preeclampsia Throughout Gestation With Maternal Characteristics and Biophysical and Biochemical Markers: A Longitudinal StudydhapitstinNo ratings yet
- Artigo 3Document7 pagesArtigo 3Cirineu NetoNo ratings yet
- 8699 36053 1 PBDocument7 pages8699 36053 1 PBPatrick RamosNo ratings yet
- 2015 Embryos, DOHaD and David BarkerDocument7 pages2015 Embryos, DOHaD and David BarkerNguyễn Tiến HồngNo ratings yet
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Document21 pagesGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguNo ratings yet
- Sibai PDFDocument2 pagesSibai PDFAdriana PajueloNo ratings yet
- Identification of IUGR via Cord Blood and Neonatal Serum BiomarkersDocument1 pageIdentification of IUGR via Cord Blood and Neonatal Serum BiomarkersWijitha VarenniNo ratings yet
- Ultrasound in Obstet Gyne - 2022 - Giorgione - Routine First Trimester Pre Eclampsia Screening and Risk of Preterm BirthDocument7 pagesUltrasound in Obstet Gyne - 2022 - Giorgione - Routine First Trimester Pre Eclampsia Screening and Risk of Preterm Birthganesh reddyNo ratings yet
- Taiwanese Journal of Obstetrics & Gynecology: Ching-Ju Shen, Shih-Han Wang, Chien-Hung Lee, Te-Fu ChanDocument4 pagesTaiwanese Journal of Obstetrics & Gynecology: Ching-Ju Shen, Shih-Han Wang, Chien-Hung Lee, Te-Fu ChanIman Ru-ancaNo ratings yet
- App Acog 2012Document10 pagesApp Acog 2012jimedureyNo ratings yet
- 2012 Pediatric Department Research DayDocument33 pages2012 Pediatric Department Research DayPayzar Wahyudi GcNo ratings yet
- Altered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVDocument17 pagesAltered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVMuhammad Pebri Nilhakim ZavbmNo ratings yet
- Mihu 2015Document7 pagesMihu 2015Nuryasni NuryasniNo ratings yet
- Impact of Paternal Age On EmbryologyDocument7 pagesImpact of Paternal Age On EmbryologyMạc Đình Cẩm TúNo ratings yet
- 61 Goepfert2004Document7 pages61 Goepfert2004angela_karenina_1No ratings yet
- Nascimento Et Al. - 2012 - Bloody Nipple Discharge in Infancy - Report of Two CasesDocument3 pagesNascimento Et Al. - 2012 - Bloody Nipple Discharge in Infancy - Report of Two CasesflashjetNo ratings yet
- 1 s2.0 S0925443918304861 MainDocument8 pages1 s2.0 S0925443918304861 MainRobert NanNo ratings yet
- 1 s2.0 S2589933319301247 MainDocument16 pages1 s2.0 S2589933319301247 MainLaura LópezNo ratings yet
- Competing Risks Model in Screening For Preeclampsia by Maternal Factors and Biomarkers at 11-13 Weeks GestationDocument12 pagesCompeting Risks Model in Screening For Preeclampsia by Maternal Factors and Biomarkers at 11-13 Weeks GestationmochkurniawanNo ratings yet
- Laborinduction: Areviewof Currentmethods: Mildred M. RamirezDocument11 pagesLaborinduction: Areviewof Currentmethods: Mildred M. RamirezRolando DiazNo ratings yet
- The NeoUpdates - DecDocument7 pagesThe NeoUpdates - DecDr Satish MishraNo ratings yet
- PROM Management and OutcomesDocument6 pagesPROM Management and OutcomesRayhan AlatasNo ratings yet
- PCOSDocument9 pagesPCOSirmaNo ratings yet
- Maternal Probiotic Supplementation May Influence Cord Blood Cytokines and Breast Milk FactorsDocument9 pagesMaternal Probiotic Supplementation May Influence Cord Blood Cytokines and Breast Milk FactorsSarfrazNo ratings yet
- Endometrial Gene Expression: An Emerging Paradigm for Reproductive DisordersFrom EverandEndometrial Gene Expression: An Emerging Paradigm for Reproductive DisordersJoanne Kwak-KimNo ratings yet
- Phasing With MRDocument95 pagesPhasing With MRLívia DantasNo ratings yet
- Race and EthnicityDocument3 pagesRace and EthnicityIvan VazquezNo ratings yet
- American Embryo Transfer Association: Certification Program GuidelinesDocument8 pagesAmerican Embryo Transfer Association: Certification Program GuidelinesFelipe MendozaNo ratings yet
- JurnalDocument10 pagesJurnalIca PurnamasariNo ratings yet
- Ceramides and Barrier Function in Healthy Skin: Investigative ReportDocument4 pagesCeramides and Barrier Function in Healthy Skin: Investigative Reportamelia080589No ratings yet
- Kar Gut Kar 2017Document9 pagesKar Gut Kar 2017Fake TomNo ratings yet
- Muscular SystemDocument5 pagesMuscular SystemBNo ratings yet
- Myers AP 3e - Unit 3 - WatermarkDocument78 pagesMyers AP 3e - Unit 3 - WatermarkRahaf AftanNo ratings yet
- Anti AIDS HerbsDocument6 pagesAnti AIDS Herbskhansa maryamNo ratings yet
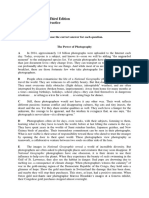
- Reading Explorer 4, Third Edition Additional Reading Practice Unit 1BDocument29 pagesReading Explorer 4, Third Edition Additional Reading Practice Unit 1B응애No ratings yet
- Introduction BioinformaticsDocument155 pagesIntroduction BioinformaticsMarcus Barros BragaNo ratings yet
- Language Isolates and Their Genetic IdenDocument3 pagesLanguage Isolates and Their Genetic IdenGirawa KandaNo ratings yet
- Ch. 25 Body Defence MechanismsDocument34 pagesCh. 25 Body Defence Mechanisms吴昊No ratings yet
- Dwnload Full Medical Terminology For Health Professions 7th Edition Ehrlich Test Bank PDFDocument36 pagesDwnload Full Medical Terminology For Health Professions 7th Edition Ehrlich Test Bank PDFmarchingpalmerbabg100% (9)
- Laach: Important InstructionsDocument24 pagesLaach: Important InstructionsAishwarya KathareNo ratings yet
- Biology: University of Cambridge International Examinations General Certificate of Education Advanced LevelDocument8 pagesBiology: University of Cambridge International Examinations General Certificate of Education Advanced LevelwegdanNo ratings yet
- Antepartum HaemorrhageDocument18 pagesAntepartum HaemorrhageOjambo Flavia100% (1)
- Experiment No. 3 - ProteinsDocument7 pagesExperiment No. 3 - Proteinskat films “Kat”No ratings yet
- S5LT 11f 6Document8 pagesS5LT 11f 6Kristine Joy PitaNo ratings yet
- 20 Amino Acids in Human ProteinDocument2 pages20 Amino Acids in Human Proteinpanomo nasabyNo ratings yet
- Plants and EnvironmentDocument284 pagesPlants and EnvironmentYen LeNo ratings yet
- Geometric morphometrics of OsteostraciDocument7 pagesGeometric morphometrics of OsteostraciMarcela ParedesNo ratings yet
- Queen of Philippine Orchids - The Rare and Beautiful Waling-waling FlowerDocument4 pagesQueen of Philippine Orchids - The Rare and Beautiful Waling-waling FlowerWendy BalaodNo ratings yet
- IP DP PSOW - Master ListDocument10 pagesIP DP PSOW - Master ListsilviaNo ratings yet
- Philippine Threatened Fauna Booklet Volume 1 PDFDocument120 pagesPhilippine Threatened Fauna Booklet Volume 1 PDFAloy DuyaNo ratings yet
- Acceptability: ©WHO/Sergey VolkovDocument26 pagesAcceptability: ©WHO/Sergey VolkovBeatriz PatricioNo ratings yet
- Bmich 2Document1 pageBmich 2umahsuthanNo ratings yet
- Jurnal 14 - SkripsiDocument5 pagesJurnal 14 - SkripsiBagusSatriyaNo ratings yet
- Introduction to Neural Network Applications in Image ProcessingDocument12 pagesIntroduction to Neural Network Applications in Image ProcessingKornelius NdruruNo ratings yet
- Spectral Subdivisión of Limestone Types - Robert L. FolkDocument23 pagesSpectral Subdivisión of Limestone Types - Robert L. Folknsantillan7742No ratings yet