You might also like
- MaleriaDocument41 pagesMaleriadeepak_143No ratings yet
- Malaria: Malariae. Recently, It Has Been Recognized That P. Knowlesi, A Type of Malaria That NaturallyDocument32 pagesMalaria: Malariae. Recently, It Has Been Recognized That P. Knowlesi, A Type of Malaria That NaturallyFernanda DalyNo ratings yet
- Full Note On MalariaDocument23 pagesFull Note On MalariaSamuel Obeng100% (3)
- Biology Investigatory ProjectDocument15 pagesBiology Investigatory ProjectVikas Ojha69% (16)
- Effects of Mobile PhonesDocument7 pagesEffects of Mobile PhonesKristine YoungNo ratings yet
- Sex-Determination System - WikipediaDocument61 pagesSex-Determination System - WikipediaDeepak maliNo ratings yet
- PROJECTDocument20 pagesPROJECTTechTalkNo ratings yet
- Thesis M.sc. MicrobiologyDocument40 pagesThesis M.sc. MicrobiologyMohit Agarwal100% (1)
- The Morphology of The Post-Gastric Alimentary CanalDocument18 pagesThe Morphology of The Post-Gastric Alimentary CanalAnca MihalcescuNo ratings yet
- Pollution PPT 090720025050 Phpapp02Document31 pagesPollution PPT 090720025050 Phpapp02anmolNo ratings yet
- Teeth New PDFDocument21 pagesTeeth New PDFavinashNo ratings yet
- Project On Malaria 1Document9 pagesProject On Malaria 1Ankur BhatiaNo ratings yet
- On Malaria AdarshDocument11 pagesOn Malaria Adarshadarsh25% (4)
- Impact of Agricultural Sector On Indian EconomyDocument17 pagesImpact of Agricultural Sector On Indian EconomyAmit Dandapath100% (6)
- Project Report On MalnutritionDocument8 pagesProject Report On MalnutritionRahul Krishnan0% (1)
- Tuberculosis Project Report pdf3 PDFDocument35 pagesTuberculosis Project Report pdf3 PDFpari bNo ratings yet
- Navjaat Shishu Suraksha Karyakram: Training ManualDocument99 pagesNavjaat Shishu Suraksha Karyakram: Training ManualBiswaranjan Padhy100% (1)
- Nutritional - Pregnant WomenDocument44 pagesNutritional - Pregnant WomenGodfred AbleduNo ratings yet
- Kap QuestionnaireDocument10 pagesKap QuestionnaireSowmi AnitaNo ratings yet
- Project On AidsDocument7 pagesProject On AidsRoshanGS20% (5)
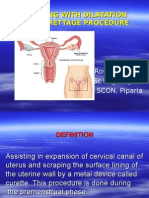
- Assisting With Dilatation and Curettage ProcedureDocument18 pagesAssisting With Dilatation and Curettage ProcedureRoselineTiggaNo ratings yet
- Dengue Fever: A Project Report ONDocument61 pagesDengue Fever: A Project Report ONShreyanshi VermaNo ratings yet
- Screenshot 2023-09-05 at 9.24.20 PMDocument17 pagesScreenshot 2023-09-05 at 9.24.20 PMThanvi EraparajuNo ratings yet
- Project of ThalassemiaDocument10 pagesProject of ThalassemiaOsama ALGabriNo ratings yet
- Microbiology Project TopicsDocument3 pagesMicrobiology Project TopicsGabriel Ken100% (1)
- Global Burden of DiseasesDocument14 pagesGlobal Burden of DiseasessarahNo ratings yet
- Malaria Best Investigatory ProjectDocument37 pagesMalaria Best Investigatory ProjectDivyansh PandeyNo ratings yet
- Nosocomial InfectionDocument18 pagesNosocomial InfectionLibérée Rumagihwa100% (1)
- ICDSDocument18 pagesICDSSreekanth ReddyNo ratings yet
- NIBEDITA SAHU-final ThesisDocument78 pagesNIBEDITA SAHU-final ThesisSuman AgrawalNo ratings yet
- National Vector Borne Disease Control ProgrammeDocument100 pagesNational Vector Borne Disease Control ProgrammeThe ThemerNo ratings yet
- Biology Project 2018-19: Topic: Aids and Hiv BY Mohammad Farhan CLASS-12-A ROLL NO.Document19 pagesBiology Project 2018-19: Topic: Aids and Hiv BY Mohammad Farhan CLASS-12-A ROLL NO.Md Raju100% (3)
- Project ReportDocument41 pagesProject ReportAnoop PunathilNo ratings yet
- Ayushman BharatDocument29 pagesAyushman BharatKailash Nagar0% (1)
- Reproductive Health SK SinghDocument31 pagesReproductive Health SK SinghKUNAL KISHORENo ratings yet
- The Prevalence of Malaria Among Pregnant Women On Addmission in Imo State Specialist Hospital OwerriDocument34 pagesThe Prevalence of Malaria Among Pregnant Women On Addmission in Imo State Specialist Hospital OwerriDaniel ObasiNo ratings yet
- Nanotechnology (Seminar)Document17 pagesNanotechnology (Seminar)TB100% (5)
- Health Problem in IndiaDocument35 pagesHealth Problem in IndiaLokesh patelNo ratings yet
- Prevalence of Malaria in Ghana: A Case Study of The Bosomtwe-Atwima Kwawoma District in The Ashanti Region.Document58 pagesPrevalence of Malaria in Ghana: A Case Study of The Bosomtwe-Atwima Kwawoma District in The Ashanti Region.benny26ghNo ratings yet
- Investigatory Project BiologyDocument6 pagesInvestigatory Project BiologykavyaNo ratings yet
- PlagueDocument20 pagesPlagueHemanth G.No ratings yet
- Zoology Project On Butterfly ?Document66 pagesZoology Project On Butterfly ?kanha creations With kanha100% (1)
- "Automatic Leaf Disease Classifier": Visvesvaraya Technological University Jnana Sangama, Belagavi - 590018Document58 pages"Automatic Leaf Disease Classifier": Visvesvaraya Technological University Jnana Sangama, Belagavi - 590018Anand TamilarasanNo ratings yet
- Agriculture in India Issues and ChallengesDocument9 pagesAgriculture in India Issues and ChallengesAkhil SatheeshNo ratings yet
- National Health ProgrammesDocument52 pagesNational Health ProgrammesZaina AkramNo ratings yet
- Computer in EpidemiologyDocument30 pagesComputer in Epidemiologysolomon rimamchirikaNo ratings yet
- ChemistryDocument17 pagesChemistrySanjay soniNo ratings yet
- Batch-5 IOT Enabled Air Pollution Monitoring SystemDocument44 pagesBatch-5 IOT Enabled Air Pollution Monitoring SystemSreevani GaddamNo ratings yet
- Disease Prediction Using Machine Learning Over Big DataDocument8 pagesDisease Prediction Using Machine Learning Over Big Datacaijjournal2No ratings yet
- Sericulture - FormattedDocument18 pagesSericulture - FormattedllldNo ratings yet
- New Telemedicine-1Document9 pagesNew Telemedicine-1Martha0% (1)
- Diabetes ProjectDocument12 pagesDiabetes ProjectrollyNo ratings yet
- Hospital Management Mba ProjectDocument69 pagesHospital Management Mba ProjectSrk SivaramakrishnanNo ratings yet
- There Are Four Types of MalariaDocument5 pagesThere Are Four Types of MalariaSatish GuptaNo ratings yet
- Malaria - MayoClinic PDFDocument6 pagesMalaria - MayoClinic PDFAdreiTheTripleANo ratings yet
- Malaria: Nama: Rismawati NIM: C 111 09 752Document6 pagesMalaria: Nama: Rismawati NIM: C 111 09 752Rismawati AcenkNo ratings yet
- MalariaDocument11 pagesMalariaGaro AllieNo ratings yet
- MalariaDocument6 pagesMalariaBrandon GarciaNo ratings yet
- Swine Flu: Diseasealso Called Swine Influenza, Influenza A (H1N1), Hog Flu, or Pig FluDocument9 pagesSwine Flu: Diseasealso Called Swine Influenza, Influenza A (H1N1), Hog Flu, or Pig FluSarvesh JaiswalNo ratings yet
- Leishmaniasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeishmaniasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- CPRDocument53 pagesCPRasutoshNo ratings yet
- Project On Child CareDocument54 pagesProject On Child CareasutoshNo ratings yet
- About Company: AknowledgementDocument3 pagesAbout Company: AknowledgementasutoshNo ratings yet
- Fron Page Thesis Sharad SirDocument2 pagesFron Page Thesis Sharad SirasutoshNo ratings yet
- Executive SummaryDocument3 pagesExecutive SummaryasutoshNo ratings yet
- Bachelor of Science in Project and Facility Management With Honours MAY 2020Document17 pagesBachelor of Science in Project and Facility Management With Honours MAY 2020Suziah Baindis AngkimNo ratings yet
- Role of NeuropsychologistDocument15 pagesRole of NeuropsychologistMahnoor MalikNo ratings yet
- PEDIATRIC Blunt Abdominal Injury MGMT Guidelines AlgorithmDocument6 pagesPEDIATRIC Blunt Abdominal Injury MGMT Guidelines AlgorithmHaidir MuhammadNo ratings yet
- Piet AlDocument6 pagesPiet AlKiara NurmathiasNo ratings yet
- Masks PhilipsDocument13 pagesMasks PhilipsMedSparkNo ratings yet
- The Occasional Intubator: by DR Minh Le Cong RFDS Cairns, April 2011Document55 pagesThe Occasional Intubator: by DR Minh Le Cong RFDS Cairns, April 2011carlodapNo ratings yet
- Genital Tract InjuriesDocument24 pagesGenital Tract InjuriesManisha ThakurNo ratings yet
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- HDL (Good) Cholesterol - HDL Stands For High-Density Lipoproteins. These AreDocument10 pagesHDL (Good) Cholesterol - HDL Stands For High-Density Lipoproteins. These ArenaliniNo ratings yet
- Shoulder Problems / Shoulder Injuries in RugbyDocument10 pagesShoulder Problems / Shoulder Injuries in RugbyAvinash NithyanandNo ratings yet
- Final Past Papers With Common MCQS: MedicineDocument17 pagesFinal Past Papers With Common MCQS: MedicineKasun PereraNo ratings yet
- (MRSA) InfectionDocument21 pages(MRSA) InfectionKhurram NadeemNo ratings yet
- Position S: Pratiksha RaiDocument49 pagesPosition S: Pratiksha RaiJoanne Cristie TolopiaNo ratings yet
- GOING TO THE DOCTOR (Body and Health) : VocabularyDocument2 pagesGOING TO THE DOCTOR (Body and Health) : VocabularyDiana CuleaNo ratings yet
- Terapi Cairain Dan ElektrolitDocument39 pagesTerapi Cairain Dan ElektrolityulyaNo ratings yet
- Managing Orthopaedics at Rittenhouse Medical CenterDocument19 pagesManaging Orthopaedics at Rittenhouse Medical CenterSyeda AqsaNo ratings yet
- IMCIDocument27 pagesIMCImesdejen100% (6)
- Anesthesia Books 2016 BLS BasicDocument5 pagesAnesthesia Books 2016 BLS BasicVinay KumarNo ratings yet
- Know Your Blood Sugar Numbers PDFDocument2 pagesKnow Your Blood Sugar Numbers PDFeliNo ratings yet
- 1428567842PE-Perianal Fistula - GS - PE.01.0711Document2 pages1428567842PE-Perianal Fistula - GS - PE.01.0711Ronal GopeNo ratings yet
- Metals and Psychotherapy - Rudolf Treichler (AnthroMed)Document6 pagesMetals and Psychotherapy - Rudolf Treichler (AnthroMed)Alexandre Funcia100% (1)
- Phocomelia: A Case Study: March 2014Document3 pagesPhocomelia: A Case Study: March 2014Nexi anessaNo ratings yet
- Assoc. Prof. Ma. Jennifer R. Tiburcio, MSMT Department of Med Tech UST Faculty of PharmacyDocument27 pagesAssoc. Prof. Ma. Jennifer R. Tiburcio, MSMT Department of Med Tech UST Faculty of PharmacyJaellah MatawaNo ratings yet
- Sleep Apnea PDFDocument257 pagesSleep Apnea PDFdantevermillion100% (6)
- Francis N. Ramirez, MDDocument9 pagesFrancis N. Ramirez, MDPridas GidNo ratings yet
- Kode ICD 10Document111 pagesKode ICD 10MarnitaNo ratings yet
- Medication Information For Parents and Teachers: Atomoxetine-StratteraDocument8 pagesMedication Information For Parents and Teachers: Atomoxetine-StratteraMonique WrightNo ratings yet
- 1 Thyroid Profile Free - PO1593405471 707Document1 page1 Thyroid Profile Free - PO1593405471 707TanmoyNo ratings yet
- Rosuvastatin: Role in Secondary Prevention of Cardiovascular DiseaseDocument5 pagesRosuvastatin: Role in Secondary Prevention of Cardiovascular Diseasenasir uddinNo ratings yet
- Bedside Techniques Methods of Clinical Xamination Muhammad InayatullahDocument6 pagesBedside Techniques Methods of Clinical Xamination Muhammad InayatullahAli HusnainNo ratings yet