You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sputum Culture and SensitivityDocument8 pagesSputum Culture and SensitivityMarivic DianoNo ratings yet
- VIROLOGY (Harr)Document8 pagesVIROLOGY (Harr)narissaNo ratings yet
- Pre TEST CD Set 1Document5 pagesPre TEST CD Set 1Princess Mae MagadanNo ratings yet
- Subject:-: Community Health NursingDocument18 pagesSubject:-: Community Health NursingKailash NagarNo ratings yet
- Buku Jawaban Ujian (Bju) Uas Take Home Exam (The) SEMESTER 2020/21.2 (2021.1)Document6 pagesBuku Jawaban Ujian (Bju) Uas Take Home Exam (The) SEMESTER 2020/21.2 (2021.1)Amsal GenarethNo ratings yet
- Hyperhomocysteinemia A Risk Fator For Ischemic Stroke in ChildrenDocument4 pagesHyperhomocysteinemia A Risk Fator For Ischemic Stroke in ChildrenAstri Faluna SheylavontiaNo ratings yet
- Nej Mic M 1506911Document1 pageNej Mic M 1506911Astri Faluna SheylavontiaNo ratings yet
- Fatal Amniotic Fluid Embolism With Typical Pathohistological, HistochemicalDocument5 pagesFatal Amniotic Fluid Embolism With Typical Pathohistological, HistochemicalAstri Faluna SheylavontiaNo ratings yet
- Graves Disease and The Manifestations of ThyrotoxicosisDocument77 pagesGraves Disease and The Manifestations of ThyrotoxicosisAstri Faluna SheylavontiaNo ratings yet
- Between-Hospital Variation in Treatment and Outcomes in Extremely Preterm InfantsDocument11 pagesBetween-Hospital Variation in Treatment and Outcomes in Extremely Preterm InfantsAstri Faluna SheylavontiaNo ratings yet
- Measles Virus, Immune Control, and PersistenceDocument14 pagesMeasles Virus, Immune Control, and PersistenceAstri Faluna SheylavontiaNo ratings yet
- Salmonella: DR - Vasanthi .R Professor Dept Microbiology ChriDocument52 pagesSalmonella: DR - Vasanthi .R Professor Dept Microbiology ChrividhyashreeNo ratings yet
- CovivaxDocument3 pagesCovivaxML BLNo ratings yet
- MeningitisDocument34 pagesMeningitispriska maniesNo ratings yet
- Bacterial, Viral, Polysaccharides, Recombinant and DNA VaccinesDocument15 pagesBacterial, Viral, Polysaccharides, Recombinant and DNA VaccinesAshwini_MCCNo ratings yet
- Fever Without Source: Dr. Tiroumourougane Serane. VDocument29 pagesFever Without Source: Dr. Tiroumourougane Serane. VTirouNo ratings yet
- 3 NDC2 QLJP 4 JHPacp KBEeDocument5 pages3 NDC2 QLJP 4 JHPacp KBEeSURYA PRAKASHNo ratings yet
- PDF Tablet Lepas LambatDocument13 pagesPDF Tablet Lepas Lambatannisya bubblesNo ratings yet
- CEFUROXIMEDocument1 pageCEFUROXIMEAnna LaritaNo ratings yet
- Cytomegalovirus in The Child Care SettingDocument1 pageCytomegalovirus in The Child Care Settingapi-241594325No ratings yet
- COVID-19 Compared To Other Pandemic DiseasesDocument17 pagesCOVID-19 Compared To Other Pandemic DiseasesDavid TorresNo ratings yet
- Zimbabwe TBDocument116 pagesZimbabwe TBKomalasaree KomalasareeNo ratings yet
- Gram Negative BacteriaDocument3 pagesGram Negative BacteriaAbby AitkenNo ratings yet
- Yellow FeverDocument9 pagesYellow Feversag50942723No ratings yet
- Communicable Diseases Handouts)Document15 pagesCommunicable Diseases Handouts)snpjavierNo ratings yet
- AMRDocument33 pagesAMRAbdul TawabNo ratings yet
- IMPETIGODocument10 pagesIMPETIGOafifulichwan18No ratings yet
- Malaria Skit: Script: CastDocument2 pagesMalaria Skit: Script: Castapi-26135603No ratings yet
- Leprosy in Pregnancy: Devi Noviana Saputri Surya DoriskaDocument15 pagesLeprosy in Pregnancy: Devi Noviana Saputri Surya DoriskaHardi SetiyoNo ratings yet
- Diagnosa Banding PneumoniaDocument7 pagesDiagnosa Banding PneumoniaLuphly TaluvtaNo ratings yet
- Vaksinasi Hep BDocument28 pagesVaksinasi Hep BMahasti AndrariniNo ratings yet
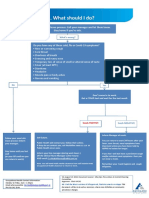
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Concepts of Plant Diseases, Diagnosis and ClassificationDocument24 pagesConcepts of Plant Diseases, Diagnosis and ClassificationNida Ratilla100% (1)
- Search Results For: Dengue: FeverDocument18 pagesSearch Results For: Dengue: FeverlakshmibavaNo ratings yet
- Cefdinir Double Dose - PIDJDocument8 pagesCefdinir Double Dose - PIDJAhmad TharwatNo ratings yet
- Rekap IMS RS Sanglah Denpasar Januari 2017Document16 pagesRekap IMS RS Sanglah Denpasar Januari 2017Ratih AndariNo ratings yet