You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Section 1 Atoms, Molecules and StoichiometryDocument27 pagesSection 1 Atoms, Molecules and Stoichiometryapi-3734333100% (2)
- Thrust Bearing CalculationsDocument162 pagesThrust Bearing Calculationslahiru1983100% (1)
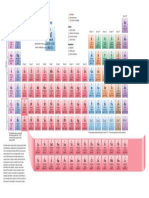
- Periodic TableDocument1 pagePeriodic TableChemist MookaNo ratings yet
- Mathematical Investigation of Trigonometric FunctionsDocument12 pagesMathematical Investigation of Trigonometric FunctionsFirasco100% (13)
- ECI Symposium Proceedings Optimizes Fouling Mitigation DesignDocument6 pagesECI Symposium Proceedings Optimizes Fouling Mitigation DesignJoseAndresCarreñoNo ratings yet
- Gas Welding and Cutting KitDocument6 pagesGas Welding and Cutting Kitkamlesh0106No ratings yet
- Ultra-Low-Power Wireless Systems - Energy-Efficient Radios For The Internet of Things PDFDocument11 pagesUltra-Low-Power Wireless Systems - Energy-Efficient Radios For The Internet of Things PDFnhatvpNo ratings yet
- P&ID ManualDocument35 pagesP&ID Manualdharan kumarNo ratings yet
- 1 - Introduction - Derivatives GreeksDocument50 pages1 - Introduction - Derivatives GreeksThomas GallantNo ratings yet
- Class XII Computer Project - Hotel ManagementDocument29 pagesClass XII Computer Project - Hotel ManagementLakshmi Puthiyedath71% (7)
- Surveying - Traverse Surveying - TraverseDocument13 pagesSurveying - Traverse Surveying - Traversebills100% (1)
- Mech Vi Non Traditional Machining (10me665) NotesDocument45 pagesMech Vi Non Traditional Machining (10me665) Notesnikhil0% (1)
- Wind Load Sheet by Abid SirDocument4 pagesWind Load Sheet by Abid SirMohammad KasimNo ratings yet
- Rational Expectation TheoryDocument7 pagesRational Expectation TheoryIsmith PokhrelNo ratings yet
- Uniform ForceDocument11 pagesUniform ForcearnoldistunoNo ratings yet
- Catalogue Inverseurs OTMDocument104 pagesCatalogue Inverseurs OTMchahbounnabil100% (1)
- LIFTING PERFORMANCE OF THE SY215C EXCAVATORDocument4 pagesLIFTING PERFORMANCE OF THE SY215C EXCAVATORAkhmad SebehNo ratings yet
- Navisworks BasicTrainingDocument54 pagesNavisworks BasicTrainingMadhankumarNo ratings yet
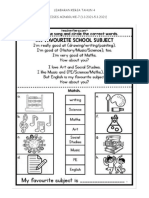
- LEMBARAN KERJA BI TAHUN 4 (m7-10) PDPRDocument9 pagesLEMBARAN KERJA BI TAHUN 4 (m7-10) PDPRnurulwaznahNo ratings yet
- Phase Shift of 180 Degrees On Reflection From Optically Denser MediumDocument1 pagePhase Shift of 180 Degrees On Reflection From Optically Denser MediumGreato HibernatoNo ratings yet
- Yokogawa 2015 Centum VP For Batch ControlDocument9 pagesYokogawa 2015 Centum VP For Batch ControlArzymanNo ratings yet
- Vector Integration - GATE Study Material in PDFDocument10 pagesVector Integration - GATE Study Material in PDFTestbook BlogNo ratings yet
- Charger Energic Plus (Catalog)Document24 pagesCharger Energic Plus (Catalog)sugar44No ratings yet
- Lecture 5 (River As A Geological Agent)Document20 pagesLecture 5 (River As A Geological Agent)Boos yousufNo ratings yet
- Notes Knouckout and BanyanDocument13 pagesNotes Knouckout and BanyanmpacNo ratings yet
- VT2009B Eng 02 953680Document2 pagesVT2009B Eng 02 953680gabrieltracto100% (1)
- Tehandler KatoDocument15 pagesTehandler KatoWalterNo ratings yet
- Solid angles in perspective: Ω, have a small but essential role in physics. For example, howDocument8 pagesSolid angles in perspective: Ω, have a small but essential role in physics. For example, howashkarkabeer08No ratings yet
- PQT MJ07Document6 pagesPQT MJ07Raguraman BalajiNo ratings yet
- Grand Vitara 2012 2013Document193 pagesGrand Vitara 2012 2013Favio Alejandro Herrera ZapataNo ratings yet