You might also like
- WikcsdsDocument2 pagesWikcsdsrmaniquez415No ratings yet
- Reden P. Maniquez AUGUST 5, 2010 BSI/T - 4B CFT Latest GadgetsDocument1 pageReden P. Maniquez AUGUST 5, 2010 BSI/T - 4B CFT Latest Gadgetsrmaniquez415No ratings yet
- EcoDocument15 pagesEcormaniquez415No ratings yet
- Recent Malware Attacks: ProcessDocument9 pagesRecent Malware Attacks: Processrmaniquez415No ratings yet
- 22Document3 pages22rmaniquez415No ratings yet
- Hon. Reden P. ManiquezDocument1 pageHon. Reden P. Maniquezrmaniquez415No ratings yet
- SOCIETY & CULTURE Final Examination 1. WhatDocument20 pagesSOCIETY & CULTURE Final Examination 1. Whatrmaniquez415No ratings yet
- RELIGION A Religion Is Any Systematic ApproachDocument14 pagesRELIGION A Religion Is Any Systematic Approachrmaniquez415No ratings yet
- SOCIETY & CULTURE Final Examination 1. WhatDocument22 pagesSOCIETY & CULTURE Final Examination 1. Whatrmaniquez415No ratings yet
- SOCIETY & CULTURE Final Examination 1. WhatDocument21 pagesSOCIETY & CULTURE Final Examination 1. Whatrmaniquez415No ratings yet
- RICHARD GORDON "Transformational Leader, The Real Action-Man"Document12 pagesRICHARD GORDON "Transformational Leader, The Real Action-Man"rmaniquez415No ratings yet
- RELIGION A Religion Is Any Systematic ApproachDocument14 pagesRELIGION A Religion Is Any Systematic Approachrmaniquez415No ratings yet
- RICHARD GORDON "Transformational Leader, The Real Action-Man"Document12 pagesRICHARD GORDON "Transformational Leader, The Real Action-Man"rmaniquez415No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Copd VS AsthmaDocument2 pagesCopd VS AsthmaHarkirat AtwalNo ratings yet
- Level of Disease PreventionDocument16 pagesLevel of Disease Preventionenam professorNo ratings yet
- SHN Learning Resource - Puberty and Menstrual HealthDocument6 pagesSHN Learning Resource - Puberty and Menstrual HealthWENNY LYN BEREDONo ratings yet
- Natural HistoryDocument55 pagesNatural HistoryPalwasha KhanNo ratings yet
- Managing Workplace Safety and HealthDocument15 pagesManaging Workplace Safety and HealthnitinmtNo ratings yet
- International Health and Safety at Work The Handbook For The NEBOSH International General Certificate 2nd Edition Paperback Routledge PDFDocument2 pagesInternational Health and Safety at Work The Handbook For The NEBOSH International General Certificate 2nd Edition Paperback Routledge PDFMohammed Mujahid0% (1)
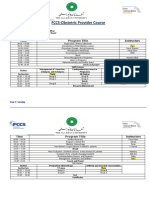
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDocument2 pagesFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNo ratings yet
- Deteksi Dini Kanker Serviks UteriDocument80 pagesDeteksi Dini Kanker Serviks UteriJULINNo ratings yet
- Pneumococcal Vaccine Timing For AdultsDocument4 pagesPneumococcal Vaccine Timing For AdultsNur Farhanah Zulkifli100% (1)
- Suggested Laboratory Specific Biosafety Manual Format: WWW - Unmc.edu/ibcDocument2 pagesSuggested Laboratory Specific Biosafety Manual Format: WWW - Unmc.edu/ibcHimanshu DarganNo ratings yet
- School Safety Assessment ToolDocument15 pagesSchool Safety Assessment ToolRyan WalatNo ratings yet
- How To Live A Healthy LifestyleDocument2 pagesHow To Live A Healthy LifestyleJocelynNo ratings yet
- APEDNN Curricular Framework in Emergency and Disaster Nursing - Sept2009Document35 pagesAPEDNN Curricular Framework in Emergency and Disaster Nursing - Sept2009janus5zu5iga5de5leonNo ratings yet
- MARCH@ NARRATIVE-REPORT-and-DocumentationDocument13 pagesMARCH@ NARRATIVE-REPORT-and-DocumentationMeriely BationNo ratings yet
- Lesson 2 Risk Management As Applied To Safety, SecurityDocument30 pagesLesson 2 Risk Management As Applied To Safety, SecurityMarlon AndayaNo ratings yet
- DiarrheaDocument28 pagesDiarrheakalpesh parvatNo ratings yet
- The Effects of Cigarette Smoking To The Health of Automotive Grade 11 and Grade 12 Students in Computer Reseacrh Network, INC Background of The StudyDocument9 pagesThe Effects of Cigarette Smoking To The Health of Automotive Grade 11 and Grade 12 Students in Computer Reseacrh Network, INC Background of The StudyRuel OrculloNo ratings yet
- Principles of Management of MDR-TBDocument22 pagesPrinciples of Management of MDR-TBGeorge VergheseNo ratings yet
- Ijobs ListDocument460 pagesIjobs ListGazetteonline100% (1)
- Sep Tank DesignDocument36 pagesSep Tank Designsrinivasakannan23No ratings yet
- Women's Health: HysterectomyDocument7 pagesWomen's Health: HysterectomySuci RahmayeniNo ratings yet
- Healthcare Associated Infections in The Nicu PowerpointDocument21 pagesHealthcare Associated Infections in The Nicu Powerpointapi-489132887No ratings yet
- CHNDocument49 pagesCHNAlbert Remollo Jr100% (2)
- Maternal Safety Bundle For: Severe Hypertension in PregnancyDocument34 pagesMaternal Safety Bundle For: Severe Hypertension in PregnancyCarlos MayaNo ratings yet
- Personal StatementsDocument18 pagesPersonal StatementsVenkatesh GorurNo ratings yet
- Bioresource Technology: Dean O. CliverDocument3 pagesBioresource Technology: Dean O. CliverPrathameshNo ratings yet
- Prev de Gingivitis Y... Salud (I) Ciencia 2015 PDFDocument6 pagesPrev de Gingivitis Y... Salud (I) Ciencia 2015 PDFCelia LinaresNo ratings yet
- Donning and DoffingDocument4 pagesDonning and DoffingAbegail QuintoNo ratings yet
- Experts Validation TableDocument20 pagesExperts Validation TableDeepti KukretiNo ratings yet
- Immunization Schedule, Japan Vaccination JaponDocument1 pageImmunization Schedule, Japan Vaccination JaponBouissac100% (2)