You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Older Adults and Integrated Health Settings: Opportunities and Challenges For Mental Health CounselorsDocument15 pagesOlder Adults and Integrated Health Settings: Opportunities and Challenges For Mental Health CounselorsGabriela SanchezNo ratings yet
- Content Mental/Behavioral Health Services: Medicaid Home and Community-Based Servicest ServerDocument15 pagesContent Mental/Behavioral Health Services: Medicaid Home and Community-Based Servicest ServerGabriela SanchezNo ratings yet
- Integrating Health and Wellness in Mental Health Counseling: Clinical, Educational, and Policy ImplicationsDocument13 pagesIntegrating Health and Wellness in Mental Health Counseling: Clinical, Educational, and Policy ImplicationsGabriela Sanchez100% (1)
- Short StoryDocument3 pagesShort StoryGabriela SanchezNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CBSE JEE(Main) 2015 admit card for Jose Daniel GumpulaDocument1 pageCBSE JEE(Main) 2015 admit card for Jose Daniel GumpulaSuman BabuNo ratings yet
- Philippine Higher Education Landscape and ReformsDocument41 pagesPhilippine Higher Education Landscape and Reformsjayric atayanNo ratings yet
- Principles of Montessori MethodDocument2 pagesPrinciples of Montessori MethodIqra Montessori100% (5)
- Lesson Plan 2016-17Document10 pagesLesson Plan 2016-17api-356400139No ratings yet
- RP Assignment BriefDocument3 pagesRP Assignment BriefishmeetvigNo ratings yet
- Learning Styles: Knowing How You Learn Can Make All The DifferenceDocument9 pagesLearning Styles: Knowing How You Learn Can Make All The DifferenceCdz Ju LaiNo ratings yet
- RPMS PURPLE TEMPLATE For MALE TEACHERS - Results-Based-Performance-Management-SystemDocument46 pagesRPMS PURPLE TEMPLATE For MALE TEACHERS - Results-Based-Performance-Management-SystemFretzelle Hope BadoyNo ratings yet
- Graphic Organizer Concept AttainmentDocument1 pageGraphic Organizer Concept Attainmentapi-272175470No ratings yet
- Education at The Edge: Negotiating Pueblo Identity in New Mexico's Indian Boarding SchoolsDocument41 pagesEducation at The Edge: Negotiating Pueblo Identity in New Mexico's Indian Boarding SchoolsUniversity of Washington PressNo ratings yet
- 11.0 Update On OSSIDocument3 pages11.0 Update On OSSIParents' Coalition of Montgomery County, MarylandNo ratings yet
- Designing A Learning ExperienceDocument10 pagesDesigning A Learning Experienceapi-284900357No ratings yet
- Teaching & Learning BiologyDocument178 pagesTeaching & Learning BiologyobsrvrNo ratings yet
- Handbook NssDocument21 pagesHandbook NssSuresh KumarNo ratings yet
- Daily Lesson Log: Subject:21st Century Literature From The Philippines and The World DateDocument3 pagesDaily Lesson Log: Subject:21st Century Literature From The Philippines and The World DateAseret MihoNo ratings yet
- Communicative Language Teaching Approach StudyDocument78 pagesCommunicative Language Teaching Approach StudyChlea Marie Tañedo AbucejoNo ratings yet
- CHSS Reflections Spring 2020Document27 pagesCHSS Reflections Spring 2020Reza ParchizadehNo ratings yet
- The Kinds of Training Provided at OrkinDocument3 pagesThe Kinds of Training Provided at OrkinasifibaNo ratings yet
- SKILL MATRIX V 1.1Document12 pagesSKILL MATRIX V 1.1vgrkumarNo ratings yet
- Legal Bases of School AdministrationDocument5 pagesLegal Bases of School AdministrationRenalyn Lumpay AñanoNo ratings yet
- KaduwaDocument34 pagesKaduwaRohini WidyalankaraNo ratings yet
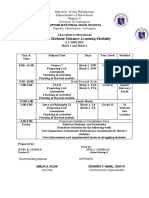
- Teachers Program Printed Modular Learning ModalityDocument2 pagesTeachers Program Printed Modular Learning ModalityCastolo Bayucot JvjcNo ratings yet
- Classifying Construction ToolsDocument1 pageClassifying Construction Toolsjoice dela cruzNo ratings yet
- Patterns Grade 1Document4 pagesPatterns Grade 1kkgreubelNo ratings yet
- An Analysis of Deaf Culture in The PhilippinesDocument28 pagesAn Analysis of Deaf Culture in The PhilippinesAngela LeeNo ratings yet
- Art 2 Unit 4Document9 pagesArt 2 Unit 4api-264152935No ratings yet
- BTEC Assignment Brief: (For NQF Only)Document4 pagesBTEC Assignment Brief: (For NQF Only)Jane KnightNo ratings yet
- UntitledDocument6 pagesUntitledapi-142797433No ratings yet
- T LE 9 June 3Document9 pagesT LE 9 June 3Ellise DanielleNo ratings yet
- COT - RPMS: Teacher I-Iii Rating SheetDocument2 pagesCOT - RPMS: Teacher I-Iii Rating Sheetceledonio borricano.jrNo ratings yet
- Vocabluary 1 (Speakout 2nd Intermediate)Document3 pagesVocabluary 1 (Speakout 2nd Intermediate)Olga KohnoNo ratings yet