You might also like
- Pharm DR Ahmed Abd AlrahmanDocument24 pagesPharm DR Ahmed Abd AlrahmanAmrAliTahaNo ratings yet
- Micro Buzz Words - KEY WordsDocument8 pagesMicro Buzz Words - KEY WordsKris GulleyNo ratings yet
- CS MnemonicsDocument7 pagesCS MnemonicsRohail MalikNo ratings yet
- AntimicrobialsDocument1 pageAntimicrobialsRomaine Barrett100% (1)
- First Aid MnemonicsDocument27 pagesFirst Aid MnemonicsRafael G. Garcia SanchezNo ratings yet
- Usmle Step 1 Terms ResumeDocument16 pagesUsmle Step 1 Terms ResumeJorge Luis LopezNo ratings yet
- Hematology & Oncology FirecrackerDocument91 pagesHematology & Oncology FirecrackerMiri PravdaNo ratings yet
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- UW 2021 Notes - Lungs UsmleDocument422 pagesUW 2021 Notes - Lungs Usmlekathi raja sekhar100% (1)
- HematologyDocument182 pagesHematologyXimena GómezNo ratings yet
- Second Aid - USMLE MnemonicsDocument21 pagesSecond Aid - USMLE MnemonicsKgerbNo ratings yet
- Biochemisty Cheat SheetsDocument4 pagesBiochemisty Cheat SheetsNatalie KingNo ratings yet
- USMLE STEP 1: Microbiology Bug List With Drugs Bugs Drugs: Bacteriology BacteriologyDocument4 pagesUSMLE STEP 1: Microbiology Bug List With Drugs Bugs Drugs: Bacteriology BacteriologymkhararahNo ratings yet
- Brenner and Stevens, Pharmacology 3 © 2010Document5 pagesBrenner and Stevens, Pharmacology 3 © 2010PharAwayNo ratings yet
- HY Endocrine UsmleDocument22 pagesHY Endocrine UsmleNakhal JararNo ratings yet
- FA MenominicsDocument43 pagesFA MenominicssarahNo ratings yet
- USMLE Step 1 DrugsDocument36 pagesUSMLE Step 1 DrugscougardiverNo ratings yet
- USMLE Step 1 NotesDocument5 pagesUSMLE Step 1 NotesvillarexNo ratings yet
- Lippin NotesDocument8 pagesLippin Noteswalt65100% (1)
- Sketchy WordDocument9 pagesSketchy WordPäw Yusoph100% (1)
- Penicillins Pen&G Pen&V: T.%pallidum% (Syphilis)Document1 pagePenicillins Pen&G Pen&V: T.%pallidum% (Syphilis)gregoryvo100% (5)
- Picmonic Glycogen Storage DiseasesDocument2 pagesPicmonic Glycogen Storage DiseasesLaylee Clare100% (3)
- Renal Chart 2Document21 pagesRenal Chart 2fortheloveofmedicineNo ratings yet
- Diseases and Deficiencies - USMLE / COMLEXDocument15 pagesDiseases and Deficiencies - USMLE / COMLEXtNo ratings yet
- Usmle QDocument46 pagesUsmle QRoh Jiten100% (1)
- Renal CastsDocument1 pageRenal Castsgregoryvo100% (4)
- High Yields Fact From UWORLDDocument6 pagesHigh Yields Fact From UWORLDBang QuachNo ratings yet
- Goljan Transcribed NotesDocument59 pagesGoljan Transcribed NotesJiyeon JeonNo ratings yet
- What I MadeDocument284 pagesWhat I MadenehaNo ratings yet
- USMLE STEP 1 CHECKLIST @lifeinwhitecoatDocument23 pagesUSMLE STEP 1 CHECKLIST @lifeinwhitecoatGlorivy E. Mora Gonzalez100% (3)
- Antibiotic Sensitivity FINAL V4 Sheet1Document1 pageAntibiotic Sensitivity FINAL V4 Sheet1JHNo ratings yet
- IM Part 1 and 2 CombinedDocument100 pagesIM Part 1 and 2 CombinedsasghfdgNo ratings yet
- Revised PPClues - 3-3-08Document16 pagesRevised PPClues - 3-3-08jeffjohnson909100% (2)
- USMLE Flashcards: Microbiology and Immunology - Side by SideDocument196 pagesUSMLE Flashcards: Microbiology and Immunology - Side by SideMedSchoolStuff0% (1)
- Diseases - BiochemDocument4 pagesDiseases - BiochemJay FeldmanNo ratings yet
- AV UWorld EOs (Rough Draft) - Data - QID LandscapeDocument139 pagesAV UWorld EOs (Rough Draft) - Data - QID LandscapeFeroz RaZa SoomrOo100% (2)
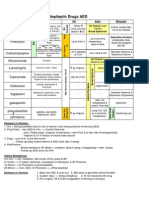
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Micro Not in SketchyDocument4 pagesMicro Not in Sketchyrpascua123No ratings yet
- Diseases in PicsDocument57 pagesDiseases in Picsapi-3840195No ratings yet
- Antibiotics Chart 2Document10 pagesAntibiotics Chart 2Vee MendNo ratings yet
- Revision Notes Dr. A. MowafyDocument222 pagesRevision Notes Dr. A. MowafyMohammed RisqNo ratings yet
- IVMS Hematology-Oncology Summary Table-Notes For USMLE Step 1 Prep.Document16 pagesIVMS Hematology-Oncology Summary Table-Notes For USMLE Step 1 Prep.Marc Imhotep Cray, M.D.100% (1)
- Haematology II Past Papers 3rd YearDocument11 pagesHaematology II Past Papers 3rd YearSyed Muhammad HameemNo ratings yet
- Free AssociationDocument10 pagesFree AssociationimorkzoneNo ratings yet
- USMLE Step 1 Study PlannerDocument6 pagesUSMLE Step 1 Study Plannertmtb04No ratings yet
- Pharmacology Step 1 For USMLEDocument3 pagesPharmacology Step 1 For USMLEraj_1041100% (1)
- Micro Cheat Sheet #1 For PASS ProgramDocument10 pagesMicro Cheat Sheet #1 For PASS ProgramOJOSAZULESAK100% (1)
- UW (Step 1) Renal - Educational Objectives PDFDocument50 pagesUW (Step 1) Renal - Educational Objectives PDFDrbee10No ratings yet
- Normal Lab Values (USMLE Step 1)Document12 pagesNormal Lab Values (USMLE Step 1)nmp274No ratings yet
- Biochemistry Firecracker QuestionsDocument92 pagesBiochemistry Firecracker QuestionsSatishAdvaniNo ratings yet
- Pathoma ChartsDocument73 pagesPathoma ChartsRa Vi100% (1)
- CS Blue Sheet Mnemonics - USMLE Step 2 CSDocument1 pageCS Blue Sheet Mnemonics - USMLE Step 2 CSRafael G. Garcia SanchezNo ratings yet
- Case Presentation 3 DR Oscar Laryngitis TBDocument33 pagesCase Presentation 3 DR Oscar Laryngitis TBmarajuu50% (2)
- Question BankDocument15 pagesQuestion BanksumpreronaNo ratings yet
- Spirochetes: Pantyo V., PHD Department of Microbiology, Virology, Epidemiology With Course of Infectious DiseasesDocument29 pagesSpirochetes: Pantyo V., PHD Department of Microbiology, Virology, Epidemiology With Course of Infectious DiseasesVivek Chaudhary100% (1)
- Executive Briefer EreidDocument2 pagesExecutive Briefer Ereidjohnllenalcantara50% (2)
- 11 - Anaerobic BacteriaDocument68 pages11 - Anaerobic BacteriaJohanna Kate DiestroNo ratings yet
- Approach To A Patient With ParaplegiaDocument31 pagesApproach To A Patient With ParaplegiaFaisal Qureshi75% (4)
- Image Analysis and Machine Learning For Detecting MalariaDocument21 pagesImage Analysis and Machine Learning For Detecting MalariaWilliam JonathanNo ratings yet
- Biology 9th Solving A Biological ProblemDocument5 pagesBiology 9th Solving A Biological Problemmhussainshigri786No ratings yet
- Etiology, Clinical Manifestations, and Diagnosis of Nephrotic Syndrome in Children - UpToDateDocument18 pagesEtiology, Clinical Manifestations, and Diagnosis of Nephrotic Syndrome in Children - UpToDateAngga Julyananda PradanaNo ratings yet
- Bee Propolis HandbookDocument23 pagesBee Propolis HandbookSabdono100% (1)
- Pisa Science QuestionsDocument8 pagesPisa Science QuestionsYuvi Ghaly100% (1)
- Frequency ListDocument386 pagesFrequency ListParmar Nilesh100% (1)
- Gastroenteritis in ChildrenDocument4 pagesGastroenteritis in ChildrenDennifer MadayagNo ratings yet
- Diseases With Diarrhea SyndromeDocument19 pagesDiseases With Diarrhea SyndromeManishNo ratings yet
- Blood Typing and SmearDocument11 pagesBlood Typing and SmearAffiqah Zulkefley100% (1)
- A Detailed Lesson in Plan in MapehDocument7 pagesA Detailed Lesson in Plan in MapehVia Thriss Ann SalasNo ratings yet
- SopDocument22 pagesSopSnowhyte KwakuNo ratings yet
- Azithromycin Drug StudyDocument1 pageAzithromycin Drug Studymilkv100% (6)
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDocument20 pagesDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNo ratings yet
- Blood Fluid Examination StrasingerDocument4 pagesBlood Fluid Examination StrasingerChristin SchlittNo ratings yet
- Specimen CollectionDocument44 pagesSpecimen CollectionRandySandovalNo ratings yet
- Fever of Unknown OriginDocument14 pagesFever of Unknown OriginandreaNo ratings yet
- Complement SystemDocument4 pagesComplement SystemFait HeeNo ratings yet
- Epidemiological Triad of HIV/AIDS: AgentDocument8 pagesEpidemiological Triad of HIV/AIDS: AgentRakib HossainNo ratings yet
- Dengue Journal ReportDocument45 pagesDengue Journal ReportNisvick Autriz BasulganNo ratings yet
- Biosafety and Bioethics of Biotechnology ABS-832: DR Attya Bhatti Assistant Professor Head of Department Asab-NustDocument25 pagesBiosafety and Bioethics of Biotechnology ABS-832: DR Attya Bhatti Assistant Professor Head of Department Asab-NustVoltha HerryNo ratings yet
- Annual Medical ReportDocument6 pagesAnnual Medical ReportMarvin Joseph AndalNo ratings yet
- Bfhajhgcterial Pnfeufmjgonia PosterDocument1 pageBfhajhgcterial Pnfeufmjgonia PosterRăzvan RoșcaNo ratings yet
- Cucumber Diseases - A Practical Guide To Identification & ControlDocument40 pagesCucumber Diseases - A Practical Guide To Identification & Controlbbbsharma100% (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1460)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingFrom EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingRating: 4.5 out of 5 stars4.5/5 (104)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)