You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 100 Gross Anatomy ConceptionsDocument228 pages100 Gross Anatomy Conceptionscrsoriano2011No ratings yet
- Mage The Awakening - Intruders - Encounters With The Abyss PDFDocument228 pagesMage The Awakening - Intruders - Encounters With The Abyss PDFJohnRichardWuethrich100% (2)
- Comparative Animal Physiology: A Guide to Thermoregulation and MetabolismDocument7 pagesComparative Animal Physiology: A Guide to Thermoregulation and MetabolismWwwanand111No ratings yet
- Mclaughlin Bennett System 4 0 User GuideDocument12 pagesMclaughlin Bennett System 4 0 User Guidegirl33100% (1)
- Horizontal Bone AugmentationDocument28 pagesHorizontal Bone Augmentationgirl33No ratings yet
- Dental Cone Beam Computed Tomography PDFDocument11 pagesDental Cone Beam Computed Tomography PDFgirl33No ratings yet
- Zygomatic Implants PDFDocument18 pagesZygomatic Implants PDFgirl33No ratings yet
- Etiology and Treatment of Periapical Lesions Around Dental Implants PDFDocument8 pagesEtiology and Treatment of Periapical Lesions Around Dental Implants PDFgirl33No ratings yet
- Sinus Floor Elevation Utilizing The PDFDocument13 pagesSinus Floor Elevation Utilizing The PDFgirl33No ratings yet
- Guided Surgery - Accuracy Andefficacy PDFDocument19 pagesGuided Surgery - Accuracy Andefficacy PDFgirl33No ratings yet
- Different Techniques of Static - Dynamic Guided Implant Surgery PDFDocument14 pagesDifferent Techniques of Static - Dynamic Guided Implant Surgery PDFgirl330% (1)
- Critical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFDocument13 pagesCritical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFgirl33No ratings yet
- Short Implant in Limited Bone Volume PDFDocument25 pagesShort Implant in Limited Bone Volume PDFgirl330% (1)
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDocument19 pagesManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33No ratings yet
- Neurovascular Disturbances After Implant Surgery PDFDocument15 pagesNeurovascular Disturbances After Implant Surgery PDFgirl33No ratings yet
- Implant-Assisted Complete Prostheses PDFDocument13 pagesImplant-Assisted Complete Prostheses PDFgirl33No ratings yet
- Implant Therapy - 40 Years of ExperienceDocument6 pagesImplant Therapy - 40 Years of Experiencegirl33No ratings yet
- Classification of Angle Class III MalocclusionDocument11 pagesClassification of Angle Class III MalocclusionAnda TarasciucNo ratings yet
- Horizontal Bone AugmentationDocument28 pagesHorizontal Bone Augmentationgirl33No ratings yet
- Orto Bun 3Document12 pagesOrto Bun 3girl33No ratings yet
- Orto Bun 3Document12 pagesOrto Bun 3girl33No ratings yet
- Advances in Understanding The Urine-Concentrating MechanismDocument26 pagesAdvances in Understanding The Urine-Concentrating MechanismKiara Lopez RelaizaNo ratings yet
- GCC Customs Tariff 2017 for Live Animals & Animal ProductsDocument435 pagesGCC Customs Tariff 2017 for Live Animals & Animal ProductsColin LoboNo ratings yet
- Acetabular Fracture PostgraduateDocument47 pagesAcetabular Fracture Postgraduatekhalidelsir5100% (1)
- Lower Genital Tract InfectionDocument51 pagesLower Genital Tract InfectionSarisa SupawimonNo ratings yet
- Colonic LesionsDocument89 pagesColonic Lesionsjagadeesan_ushaNo ratings yet
- Black Wind From The Kurdish HillsDocument456 pagesBlack Wind From The Kurdish Hillstahsin azizNo ratings yet
- Action Potential of NeuronsDocument3 pagesAction Potential of NeuronscheaterxorcistNo ratings yet
- The Endangered Bambo 3Document2 pagesThe Endangered Bambo 3yejuNo ratings yet
- TigersDocument15 pagesTigersChinna MuthuNo ratings yet
- List of Collective Nouns For Birds - Animal Group NamesDocument2 pagesList of Collective Nouns For Birds - Animal Group NamesHailee Koh Shi QiNo ratings yet
- Comparative Anatomy Classification ChartDocument2 pagesComparative Anatomy Classification Chartapi-613673827No ratings yet
- (Original Size) Green & Brown Monstera Plant Fun Facts Data InfographicDocument1 page(Original Size) Green & Brown Monstera Plant Fun Facts Data InfographicMani MNo ratings yet
- Story-Telling Competition Title: The Milkmaid and Her PailDocument6 pagesStory-Telling Competition Title: The Milkmaid and Her PailCoffee&LoveNo ratings yet
- Phonetic Animals ListDocument6 pagesPhonetic Animals ListJOHN. J MESANo ratings yet
- OdomDocument31 pagesOdomRangothri Sreenivasa SubramanyamNo ratings yet
- Unleashed Pet care centreDocument38 pagesUnleashed Pet care centreSampada poteNo ratings yet
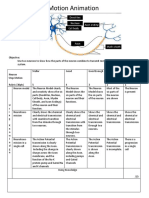
- Neurons Stop Motion AnimationDocument2 pagesNeurons Stop Motion Animationapi-495006167No ratings yet
- THE STAG - Class NotesDocument3 pagesTHE STAG - Class Notesmishka100% (1)
- 7 Principles of Leave No TraceDocument2 pages7 Principles of Leave No TraceDiether100% (1)
- 0500 - s21 - QP - 13 - May JuneDocument24 pages0500 - s21 - QP - 13 - May Juneelianwar209No ratings yet
- The LoversDocument4 pagesThe LoversabnerdormiendoNo ratings yet
- Child with noisy breathing and drooling has bronchiolitisDocument3 pagesChild with noisy breathing and drooling has bronchiolitissaudNo ratings yet
- ACUP306Document4 pagesACUP306raysklineNo ratings yet
- American ConsonantsDocument22 pagesAmerican ConsonantsAllanSalardaAdemNo ratings yet
- Kiara Maestre 2020 05 12 1420 PDFDocument2 pagesKiara Maestre 2020 05 12 1420 PDFmarionochesNo ratings yet
- Hep ADocument2 pagesHep Aapi-237098034No ratings yet
- CDC Guidelines for Disinfecting HBV, HCV, HIV, TB DevicesDocument6 pagesCDC Guidelines for Disinfecting HBV, HCV, HIV, TB Devicesmr.anggaardiantoNo ratings yet