You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Diabetes ElektifDocument7 pagesDiabetes ElektifSiti SofiaNo ratings yet
- Thyroid Disorders in ElderlyDocument16 pagesThyroid Disorders in ElderlyYayatRuslanNo ratings yet
- Diabetes: Dr. Hermawan Susanto SPPDDocument66 pagesDiabetes: Dr. Hermawan Susanto SPPDAbdur RohmanNo ratings yet
- Gluco MeterGlucometerDocument13 pagesGluco MeterGlucometerSudhanshu SharmaNo ratings yet
- Essence 8th Edition ThyroidDocument22 pagesEssence 8th Edition ThyroidMohned AlhababiNo ratings yet
- Blood Sugar Chart: Normal and Diabetic Blood Sugar RangesDocument1 pageBlood Sugar Chart: Normal and Diabetic Blood Sugar RangesBIRD MARKONo ratings yet
- Nclex Endocrine ReviewerDocument43 pagesNclex Endocrine ReviewerBryle SaladarNo ratings yet
- 3.3.cgm 09 0Document1 page3.3.cgm 09 0Jia-PeiWuNo ratings yet
- Diabetes Risk Test FreeDocument1 pageDiabetes Risk Test FreeXavier FrancaisNo ratings yet
- DAFTAR PUSTAKA DIABETES HIPOGLYKEMIADocument2 pagesDAFTAR PUSTAKA DIABETES HIPOGLYKEMIADina Ikrama PutriNo ratings yet
- Oral Hypoglycemic Drugs 16Document57 pagesOral Hypoglycemic Drugs 16daniyal kumarNo ratings yet
- Atlas of Thyroid UltrasonographyDocument399 pagesAtlas of Thyroid Ultrasonographynino.matasNo ratings yet
- Endocrine System DiseasesDocument87 pagesEndocrine System DiseasesFahmiArifMuhammadNo ratings yet
- Diabetic ComaDocument15 pagesDiabetic ComaNader Smadi100% (1)
- Hubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahDocument4 pagesHubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahFauzan MuttaqinNo ratings yet
- RBS - Random Blood Sugar PDFDocument4 pagesRBS - Random Blood Sugar PDFKrishna Faith P. DelaraNo ratings yet
- Thyroid Gland: Pactical Activity No. 5Document19 pagesThyroid Gland: Pactical Activity No. 5Damian CorinaNo ratings yet
- FSH and LH LevelsDocument4 pagesFSH and LH Levelsujjwal guptaNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument14 pagesJournal of Diabetes and Its ComplicationsZam-zam RsiNo ratings yet
- REAL in Nursing Journal (RNJ) : Relaksasi Autogenik Menurunkan Kadar Gula Darah Pasien Diabetes Melitus Tipe 2Document9 pagesREAL in Nursing Journal (RNJ) : Relaksasi Autogenik Menurunkan Kadar Gula Darah Pasien Diabetes Melitus Tipe 2gherice serumenaNo ratings yet
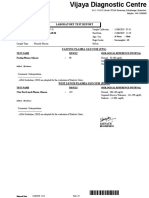
- Vijaya Diagnostic Lab Report SummaryDocument3 pagesVijaya Diagnostic Lab Report Summaryrajashekarcse533No ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- 72 Endo AnnotatedDocument9 pages72 Endo AnnotatedErika ArceoNo ratings yet
- h1 in GlucometerDocument1 pageh1 in GlucometerKepler12 QuemadaNo ratings yet
- Research Proposal - ICMR STS 2019 1. Title: Thyroid Auto-Immune Response in Pregnant Women With Gestational Diabetes Mellitus 2. ObjectiveDocument4 pagesResearch Proposal - ICMR STS 2019 1. Title: Thyroid Auto-Immune Response in Pregnant Women With Gestational Diabetes Mellitus 2. Objectivesiddarth reddyNo ratings yet
- DSSSB Je Ae Civil All 22 PapersDocument980 pagesDSSSB Je Ae Civil All 22 Papersatul meenaNo ratings yet
- Biochemical and Clinical Profile of With Diabetic Ketoacidosis: A Single Centre ExperienceDocument1 pageBiochemical and Clinical Profile of With Diabetic Ketoacidosis: A Single Centre ExperienceBianca ChiriacNo ratings yet
- 2 - 9 - KNN CodeDocument6 pages2 - 9 - KNN CodeYahya SabriNo ratings yet
- Laboratorio Clinico Toledo: Patient Number Birthdate SexDocument1 pageLaboratorio Clinico Toledo: Patient Number Birthdate SexMirle BonetNo ratings yet
- Columnar Insulin Dosing Chart : (1 ML 1 Unit)Document1 pageColumnar Insulin Dosing Chart : (1 ML 1 Unit)Philippe KinnaerNo ratings yet