You might also like
- Medical Education in Pulmonary, Critical Care, and Sleep Medicine: Advanced Concepts and StrategiesFrom EverandMedical Education in Pulmonary, Critical Care, and Sleep Medicine: Advanced Concepts and StrategiesPatricia A. KritekNo ratings yet
- Evaluation of Senior Nursing Students' Performance With High Fidelity SimulationDocument4 pagesEvaluation of Senior Nursing Students' Performance With High Fidelity SimulationJessa BorreNo ratings yet
- Factors Affecting Performance in Clinical Practice Among Preservice Diploma Nursing Students in Northern TanzaniaDocument7 pagesFactors Affecting Performance in Clinical Practice Among Preservice Diploma Nursing Students in Northern TanzaniaStel ValmoresNo ratings yet
- Research - ScriptDocument8 pagesResearch - ScriptRheizhelle Anne LaguraNo ratings yet
- International Journal of Nursing SciencesDocument5 pagesInternational Journal of Nursing SciencesWahyu Phaling FienterNo ratings yet
- CHAPTER ONE, TWO & THREE (Mallam Ibrahim)Document23 pagesCHAPTER ONE, TWO & THREE (Mallam Ibrahim)mallamsamboNo ratings yet
- Effectiveness of Related Learning Experience in Nursing Students Biostat1Document12 pagesEffectiveness of Related Learning Experience in Nursing Students Biostat1Rose Ann67% (3)
- Nres - Group 2Document25 pagesNres - Group 2charles estradaNo ratings yet
- Korean Nursing Students' Experiences of Their First Clinical PracticeDocument11 pagesKorean Nursing Students' Experiences of Their First Clinical PracticeKruh Kwabena IsaacNo ratings yet
- YeahDocument47 pagesYeahzfliezblogspotcomNo ratings yet
- Research Article: The Challenges of Nursing Students in The Clinical Learning Environment: A Qualitative StudyDocument8 pagesResearch Article: The Challenges of Nursing Students in The Clinical Learning Environment: A Qualitative StudyBreezy ReveloNo ratings yet
- Research PresentationDocument14 pagesResearch PresentationCeeNo ratings yet
- Nasarawa Conference - Clinical PracticeDocument36 pagesNasarawa Conference - Clinical PracticeyusufNo ratings yet
- Curriculum Development - Final Requirement - RemoladoDocument23 pagesCurriculum Development - Final Requirement - RemoladoJan Michael R. RemoladoNo ratings yet
- HahahahhahahahDocument13 pagesHahahahhahahahDave SoledadNo ratings yet
- Nursing EducationDocument6 pagesNursing EducationnishthaNo ratings yet
- Structured Mentoring StrategiesDocument31 pagesStructured Mentoring Strategiesrandy gallegoNo ratings yet
- Analysis of Nursing Students Clinical ExperiencesDocument6 pagesAnalysis of Nursing Students Clinical ExperiencesKruh Kwabena IsaacNo ratings yet
- Tutoría Entre Iguales en Una Escuela de Medicina Percepciones de Tutores y TutoradosDocument7 pagesTutoría Entre Iguales en Una Escuela de Medicina Percepciones de Tutores y TutoradosFalconSerfinNo ratings yet
- Reading 1Document9 pagesReading 1sisjing88510No ratings yet
- Making A Difference The Value of Preceptorship Programs in Nursing EducationDocument8 pagesMaking A Difference The Value of Preceptorship Programs in Nursing Educationsintha pratiwiNo ratings yet
- NHS PosterDocument1 pageNHS PosterPádraig Ó LúanaighNo ratings yet
- Theoretical BackgroundDocument7 pagesTheoretical BackgroundKristinelou Marie N. ReynaNo ratings yet
- Student Nurses Experience of A System of Peer GroDocument13 pagesStudent Nurses Experience of A System of Peer GroZhedriex EspirituNo ratings yet
- Guidelines On Developing A Quality Clinical Learning Environment 1st Ed. April 2003Document16 pagesGuidelines On Developing A Quality Clinical Learning Environment 1st Ed. April 2003Doyin AwodeleNo ratings yet
- Caring and Effective Teaching Behavior of Clinical Nursing Instructors in Clinical Area As Perceived by Their StudentsDocument13 pagesCaring and Effective Teaching Behavior of Clinical Nursing Instructors in Clinical Area As Perceived by Their StudentsAlexander DeckerNo ratings yet
- Naidoo Bedside TeachingDocument18 pagesNaidoo Bedside TeachingB'durNo ratings yet
- The Challenges of Nursing Students in The Clinical Learning EnvironmentDocument20 pagesThe Challenges of Nursing Students in The Clinical Learning EnvironmenthernandezmarianneroseNo ratings yet
- Clinical Care ProjectDocument7 pagesClinical Care ProjecttanvirahmedNo ratings yet
- Clinical Practice Experience by The BSN Iv Students in The Affiliated Hospitals of St. Paul University PhilippinesDocument31 pagesClinical Practice Experience by The BSN Iv Students in The Affiliated Hospitals of St. Paul University Philippinesbryiane2850% (6)
- Ijerph 17 05686Document14 pagesIjerph 17 05686Mary LowryNo ratings yet
- Effects of Simulation-Based Education On Communication Skill and Clinical Competence in Maternity Nursing PracticumDocument9 pagesEffects of Simulation-Based Education On Communication Skill and Clinical Competence in Maternity Nursing PracticumDama Trisa UtamiNo ratings yet
- Lourlyn's Angels?Document27 pagesLourlyn's Angels?lovelove DayoNo ratings yet
- OSCE Tool For Improving B. Sc. Nursing Students' Antenatal, ExaminationDocument12 pagesOSCE Tool For Improving B. Sc. Nursing Students' Antenatal, ExaminationIOSRjournalNo ratings yet
- Ramakrishna NDocument22 pagesRamakrishna NAndy Delos ReyesNo ratings yet
- Nursing and Midwifery StudentsDocument15 pagesNursing and Midwifery StudentsJumariah Tana PaserNo ratings yet
- Research Article: The Challenges of Nursing Students in The Clinical Learning Environment: A Qualitative StudyDocument8 pagesResearch Article: The Challenges of Nursing Students in The Clinical Learning Environment: A Qualitative StudyDwi Kurnia SariNo ratings yet
- Effect of High Fidelity Simulation On Clinical Decision Making Among Nursing StudentsDocument10 pagesEffect of High Fidelity Simulation On Clinical Decision Making Among Nursing Studentsاحمد العايديNo ratings yet
- Review of Related Literature (RRL) (SHEENA, BABE)Document4 pagesReview of Related Literature (RRL) (SHEENA, BABE)Nur SetsuNo ratings yet
- TOPICDocument8 pagesTOPICKeep smileNo ratings yet
- Chapter 1Document11 pagesChapter 1Yuuki Chitose (tai-kun)No ratings yet
- Improving Nursing Education :some StrategiesDocument7 pagesImproving Nursing Education :some StrategiesMary MathewsNo ratings yet
- Vol23 4-1Document6 pagesVol23 4-1fauzanhamdiNo ratings yet
- Research BriefsDocument8 pagesResearch BriefsNur MiladiyahNo ratings yet
- Correlation of The Academic and Clinical PerformanDocument10 pagesCorrelation of The Academic and Clinical PerformanissaiahnicolleNo ratings yet
- Mentoring, Nursing Students' Opinions A Pilot StudyDocument7 pagesMentoring, Nursing Students' Opinions A Pilot StudyinventionjournalsNo ratings yet
- Collaborative ModelDocument38 pagesCollaborative ModelakhilNo ratings yet
- Chapter 1 3 ResearchDocument26 pagesChapter 1 3 ResearchAb Staholic BoiiNo ratings yet
- Nurse Education Today: Ye Şim Yaman Aktaş, Neziha KarabulutDocument5 pagesNurse Education Today: Ye Şim Yaman Aktaş, Neziha Karabulut하진No ratings yet
- Adult Learnng RoleDocument13 pagesAdult Learnng RoleLoganathan ChandrasekarNo ratings yet
- Preceptor 1Document7 pagesPreceptor 1Stevanus JonathanNo ratings yet
- Research in Continuing Education Seminar Typed ContentDocument17 pagesResearch in Continuing Education Seminar Typed ContentIze C Viji93% (14)
- RRLDocument6 pagesRRLZycon Rodney Ae'zecquel GachallanNo ratings yet
- Cilar 2020Document7 pagesCilar 2020Laiza May LampadNo ratings yet
- Creating Innovation Models of Clinical Nursing Education PDFDocument6 pagesCreating Innovation Models of Clinical Nursing Education PDFallan.manaloto23No ratings yet
- The Experiences of Nurse Educators in Implementing PDFDocument9 pagesThe Experiences of Nurse Educators in Implementing PDFAPRILIYA WATINo ratings yet
- Review Article: Advanced Practice Nursing Education: Challenges and StrategiesDocument9 pagesReview Article: Advanced Practice Nursing Education: Challenges and StrategiesluNo ratings yet
- Mountain Province State Polytechnic College: School of Healthcare EducationDocument6 pagesMountain Province State Polytechnic College: School of Healthcare EducationMaller Chop's Pong-etNo ratings yet
- Student Nurses' Hand Hygiene Beliefs and Practices: Öğrenci Hemşirelerin El Hijyeni İnanç Ve UygulamalarıDocument8 pagesStudent Nurses' Hand Hygiene Beliefs and Practices: Öğrenci Hemşirelerin El Hijyeni İnanç Ve Uygulamalarısamer thaherNo ratings yet
- Rw-Omj-D-18-00175 (05C)Document6 pagesRw-Omj-D-18-00175 (05C)nersrosdianaNo ratings yet
- There Is A Family Who Have A Simple Life - But, What If Their Lives Are Change Due To Unforeseen CircumstancesDocument4 pagesThere Is A Family Who Have A Simple Life - But, What If Their Lives Are Change Due To Unforeseen CircumstancesJessa BorreNo ratings yet
- 3 Fostering Social Intellectual Creative and Emotional Development of ChildrenDocument29 pages3 Fostering Social Intellectual Creative and Emotional Development of ChildrenJessa Borre67% (9)
- Borre, Jessa Anne R. NSTP Ii Bsn-IvDocument1 pageBorre, Jessa Anne R. NSTP Ii Bsn-IvJessa BorreNo ratings yet
- Answer KeyDocument1 pageAnswer KeyJessa BorreNo ratings yet
- Significance of ResultsDocument3 pagesSignificance of ResultsJessa BorreNo ratings yet
- Board of Midwifery: Republic Act No. 7392Document12 pagesBoard of Midwifery: Republic Act No. 7392Jessa BorreNo ratings yet
- Creation Faith & EvidenceDocument3 pagesCreation Faith & EvidenceJessa BorreNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJessa BorreNo ratings yet
- Borre, Jessa Anne R. NSTP Ii Bsn-IvDocument1 pageBorre, Jessa Anne R. NSTP Ii Bsn-IvJessa BorreNo ratings yet
- Copar DocumentationDocument58 pagesCopar DocumentationJessa BorreNo ratings yet
- Cues Nursing Diagnosis Scientific Explanation Nursing Objective Nursing Intervention Scientific Explanation EvaluationDocument2 pagesCues Nursing Diagnosis Scientific Explanation Nursing Objective Nursing Intervention Scientific Explanation EvaluationJessa BorreNo ratings yet
- SSSForms Change RequestDocument9 pagesSSSForms Change RequestJessa BorreNo ratings yet
- Stressors That Affect Cognition &perception: Sensory SleepDocument35 pagesStressors That Affect Cognition &perception: Sensory SleepJessa BorreNo ratings yet
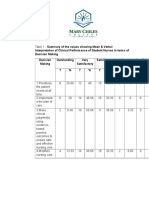
- Clinical Performance TableDocument12 pagesClinical Performance TableJessa BorreNo ratings yet
- Nursing Leadership & ManagementDocument28 pagesNursing Leadership & ManagementJessa BorreNo ratings yet
- Ambu BagDocument29 pagesAmbu BagJessa Borre100% (2)
- Jeany H. Venus Bsn-Ii Health Teaching Plan General ObjectiveDocument4 pagesJeany H. Venus Bsn-Ii Health Teaching Plan General ObjectiveJessa BorreNo ratings yet
- What Is A Critical Thinking EssayDocument7 pagesWhat Is A Critical Thinking Essayfz75nk7v100% (2)
- INSDSG Project Management For Instructional DesignersDocument16 pagesINSDSG Project Management For Instructional DesignersApostolos KoutropoulosNo ratings yet
- Stephan KörnerDocument4 pagesStephan KörnerAlan CarrollNo ratings yet
- Polytechnic University of The PhilippinesDocument6 pagesPolytechnic University of The PhilippinesChristian Kokoy C. ChuaNo ratings yet
- Urbanest Student AccomodationDocument20 pagesUrbanest Student AccomodationKarishma NarwaniNo ratings yet
- Brady Et Al 2012 CcsDocument13 pagesBrady Et Al 2012 Ccsapi-470437967No ratings yet
- How To Deconstruct A Media MessageDocument10 pagesHow To Deconstruct A Media MessageFarhan Zafar Shah100% (1)
- Multiplying Binomials Lesson Plan (Access Version)Document15 pagesMultiplying Binomials Lesson Plan (Access Version)RichardRaquenoNo ratings yet
- Alternative Indicators of Well-Being For VanuatuDocument115 pagesAlternative Indicators of Well-Being For VanuatuonibabaNo ratings yet
- Master Switchword: The EssenceDocument4 pagesMaster Switchword: The EssenceJecholiah Foli100% (4)
- Gillian Casey ResumeDocument1 pageGillian Casey ResumeGillianNo ratings yet
- Two Word UtterancesDocument18 pagesTwo Word UtterancesJames Gildardo CuasmayànNo ratings yet
- W.E.B. Du Bois (1868 - 1963) The Color LineDocument2 pagesW.E.B. Du Bois (1868 - 1963) The Color LineLola PolaNo ratings yet
- James Allen - As A Man ThinkethDocument23 pagesJames Allen - As A Man ThinkethShawn100% (4)
- FallaciesDocument12 pagesFallaciesNahyanNo ratings yet
- Estampa Ass.4 STS BSBA-OM 9.21-9.27Document4 pagesEstampa Ass.4 STS BSBA-OM 9.21-9.27Marlyn JoyNo ratings yet
- BudgetingDocument14 pagesBudgetingAngelo PeÑa ArriolaNo ratings yet
- B.A. (Hons) Staffordshire UniversityDocument9 pagesB.A. (Hons) Staffordshire UniversityshinimikageNo ratings yet
- ICSE English Language Paper 1 Question Paper (Sem 2) 2022Document2 pagesICSE English Language Paper 1 Question Paper (Sem 2) 2022jerip87163No ratings yet
- Crucible Choice Project 2016Document3 pagesCrucible Choice Project 2016api-305845489No ratings yet
- RRLDocument13 pagesRRLJerre Mae EchalarNo ratings yet
- The Lion KingDocument4 pagesThe Lion KingJasmine TanNo ratings yet
- Ray Kappe - What Makes A LegendDocument8 pagesRay Kappe - What Makes A LegendSouth Bay DigsNo ratings yet
- BILD Training Course DesignDocument19 pagesBILD Training Course DesignMary A. DillardNo ratings yet
- Masterclass of Loomis and Bargue Facial and Figure DrawingDocument5 pagesMasterclass of Loomis and Bargue Facial and Figure DrawingLuciano Carvalho100% (1)
- Self TalkDocument14 pagesSelf TalkAzizan AbasNo ratings yet
- Most Common Job Interview QuestionsDocument2 pagesMost Common Job Interview QuestionsFlavio MondragónNo ratings yet
- Ichel Cook v. Phil RomanoDocument11 pagesIchel Cook v. Phil RomanoThe Dallas Morning NewsNo ratings yet
- NBHS 1104 Topic 2Document18 pagesNBHS 1104 Topic 2hema angleNo ratings yet
- Lexical Competence (Language, Speech, and Communication)Document230 pagesLexical Competence (Language, Speech, and Communication)Kis Syn SullivanNo ratings yet