You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Asthma Control Test Nov 15Document1 pageAsthma Control Test Nov 15marizamora100% (2)
- Docosahexaenoic Acid Supplementation and Cognitive Decline in Alzheimer Disease - A Randomized TrialDocument17 pagesDocosahexaenoic Acid Supplementation and Cognitive Decline in Alzheimer Disease - A Randomized TrialmarizamoraNo ratings yet
- RPM WR2017Document102 pagesRPM WR2017marizamoraNo ratings yet
- Court upholds reinstatement of workers' claimsDocument27 pagesCourt upholds reinstatement of workers' claimsmarizamoraNo ratings yet
- Clinical Anatomy CardiovascularDocument53 pagesClinical Anatomy Cardiovascularmarizamora100% (1)
- FTKV50NVM - Operating ManualDocument20 pagesFTKV50NVM - Operating ManualmarizamoraNo ratings yet
- Aesthetic Surgery BookDocument4 pagesAesthetic Surgery BookmarizamoraNo ratings yet
- Gi Hema Onco Quiz d2012Document2 pagesGi Hema Onco Quiz d2012marizamoraNo ratings yet
- BehMed2 - Psychopharmacology20171103090642195Document187 pagesBehMed2 - Psychopharmacology20171103090642195marizamoraNo ratings yet
- Brainstem (Old Testament)Document19 pagesBrainstem (Old Testament)marizamoraNo ratings yet
- Cordycepin As A Drug ResearchDocument8 pagesCordycepin As A Drug ResearchmarizamoraNo ratings yet
- Metabolisme Asam AminoDocument27 pagesMetabolisme Asam AminoKariina Indah PrayogiNo ratings yet
- Degenerative Spine DiseasesDocument10 pagesDegenerative Spine DiseasesmarizamoraNo ratings yet
- 6 - Hypothalamus & Pituitary GlandDocument14 pages6 - Hypothalamus & Pituitary GlandmarizamoraNo ratings yet
- Spinal CordDocument2 pagesSpinal CordmarizamoraNo ratings yet
- Protein MetabolismDocument4 pagesProtein MetabolismmarizamoraNo ratings yet
- Medical CertificateDocument27 pagesMedical CertificatemarizamoraNo ratings yet
- 1001 BooksDocument19 pages1001 BooksHarshada ChaudhariNo ratings yet
- Circular 4Document4 pagesCircular 4Eli Cohen50% (2)
- cGMP and cGCP ChaptersDocument100 pagescGMP and cGCP ChaptersRahmaAulia0% (1)
- Metabolisme Asam AminoDocument27 pagesMetabolisme Asam AminoKariina Indah PrayogiNo ratings yet
- HomeostasisDocument7 pagesHomeostasismarizamoraNo ratings yet
- Ust NSTP Cwts and Lts HandbookDocument9 pagesUst NSTP Cwts and Lts HandbookJulia Mariah Codamon100% (1)
- The Mechanics of BreathingDocument12 pagesThe Mechanics of BreathingMichael SibuloNo ratings yet
- PlannerDocument1 pagePlannermarizamoraNo ratings yet
- Flash Action ScriptxDocument2 pagesFlash Action ScriptxmarizamoraNo ratings yet
- Desc MaskDocument2 pagesDesc MaskmarizamoraNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
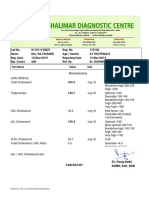
- LabreportnewDocument14 pagesLabreportnewRajesh SharmaNo ratings yet
- Go Back to Healthy Cholesterol LevelsDocument2 pagesGo Back to Healthy Cholesterol Levelsmohit kumarNo ratings yet
- Guidelines CVD Prevention AddendaDocument12 pagesGuidelines CVD Prevention AddendaJuan Sebastián Montaño MaldonadoNo ratings yet
- J. Lipid Res.-1968-Glomset-155-67Document13 pagesJ. Lipid Res.-1968-Glomset-155-67Stefania CristinaNo ratings yet
- Lipid Lowering DrugsDocument15 pagesLipid Lowering Drugsmwaithira71682No ratings yet
- Kasus 3Document18 pagesKasus 3Angga RistaNo ratings yet
- Broj 1: Zoran Tasevski Nick Naumoff Ivanco TalevskiDocument44 pagesBroj 1: Zoran Tasevski Nick Naumoff Ivanco TalevskiAleksandar StefanovskiNo ratings yet
- Case StudyDocument37 pagesCase StudyAnonymous t78m8ku100% (1)
- Understanding Cholesterol LevelsDocument5 pagesUnderstanding Cholesterol LevelsKaren ManochaNo ratings yet
- Cholesterol Factors Determining Blood Cholesterol LevelsDocument7 pagesCholesterol Factors Determining Blood Cholesterol LevelsAnonymous bKm5eCtNo ratings yet
- Multidimensional Uses of Medicinal Plantkachnar Bauhinia Variegata LinnDocument15 pagesMultidimensional Uses of Medicinal Plantkachnar Bauhinia Variegata Linnkeshav shishyaNo ratings yet
- Understanding LDL and HDL Cholesterol LevelsDocument16 pagesUnderstanding LDL and HDL Cholesterol LevelsaakashtrivediNo ratings yet
- Managing Your Cholesterol Harvard HealthDocument56 pagesManaging Your Cholesterol Harvard Healtholly fernandezNo ratings yet
- A Healthy Cholesterol 2011 Final PDFDocument20 pagesA Healthy Cholesterol 2011 Final PDFAli K SheqlawaNo ratings yet
- Max Lab ReportDocument9 pagesMax Lab ReportKallu PrasadNo ratings yet
- De La Cruz DyslipidemiaDocument87 pagesDe La Cruz DyslipidemiaKhánh ChiNo ratings yet
- HEALTHY EATING GUIDEDocument87 pagesHEALTHY EATING GUIDESamyam DahalNo ratings yet
- How To Benefit From Everyday HerbsDocument167 pagesHow To Benefit From Everyday HerbsGarcia Abdullah100% (19)
- Hypothyroidism T3 T4 Triglycerides Clinical ChemistryDocument11 pagesHypothyroidism T3 T4 Triglycerides Clinical ChemistryRitz Bautista Balanay100% (1)
- Comprehensive Medical Checkup Packages and PricesDocument12 pagesComprehensive Medical Checkup Packages and Prices91michaeljames100% (1)
- Lipid Profile Test BasicsDocument9 pagesLipid Profile Test BasicsSafooraShabbirNo ratings yet
- Gamma-Oryzanol Benefits for Lipids & MenopauseDocument10 pagesGamma-Oryzanol Benefits for Lipids & MenopauseSharif HossenNo ratings yet
- Top Drugs History, Pharmacology, Synthese (2015)Document219 pagesTop Drugs History, Pharmacology, Synthese (2015)L EPNo ratings yet
- Clinical Chemistry Quality Control GuideDocument32 pagesClinical Chemistry Quality Control GuideAnya Ignacio100% (1)
- True Control: Sero Product CatalogueDocument36 pagesTrue Control: Sero Product Catalogue陳佳華No ratings yet
- Astaxanthin Scientific Review 1006 June 2010Document106 pagesAstaxanthin Scientific Review 1006 June 2010rainmentNo ratings yet
- Nutrition Therapy For Cardiovascular DisordersDocument10 pagesNutrition Therapy For Cardiovascular DisorderspeytonNo ratings yet
- HLTH 501 Final Exam SolutionsDocument13 pagesHLTH 501 Final Exam SolutionsCarl0% (8)
- New Thesis With Corrections Grad School CorrectionsDocument62 pagesNew Thesis With Corrections Grad School Correctionsapi-535934790No ratings yet
- Lipids and MembranesDocument9 pagesLipids and MembranesPatricia Bianca BunagNo ratings yet