You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GO vs. CA Case DigestDocument1 pageGO vs. CA Case Digestunbeatable38100% (4)
- HAF F16 ManualDocument513 pagesHAF F16 Manualgreekm4dn3ss86% (7)
- Official Correspondence in English CompleteDocument55 pagesOfficial Correspondence in English Completeyadab rautNo ratings yet
- Ethical ControlDocument28 pagesEthical ControlLani Derez100% (1)
- Inmarsat M2M Terminal ComparisonDocument2 pagesInmarsat M2M Terminal Comparisonmaruka33No ratings yet
- Biological Control in Brazil An OverviewDocument10 pagesBiological Control in Brazil An OverviewGustavo Ferreira MoraisNo ratings yet
- Tahap Kesediaan Pensyarah Terhadap Penggunaan M-Pembelajaran Dalam Sistem Pendidikan Dan Latihan Teknik Dan Vokasional (TVET)Document17 pagesTahap Kesediaan Pensyarah Terhadap Penggunaan M-Pembelajaran Dalam Sistem Pendidikan Dan Latihan Teknik Dan Vokasional (TVET)Khairul Yop AzreenNo ratings yet
- Gallbladder Removal Recovery GuideDocument14 pagesGallbladder Removal Recovery GuideMarin HarabagiuNo ratings yet
- Pratt & Whitney Engine Training ResourcesDocument5 pagesPratt & Whitney Engine Training ResourcesJulio Abanto50% (2)
- International History 1900-99Document5 pagesInternational History 1900-99rizalmusthofa100% (1)
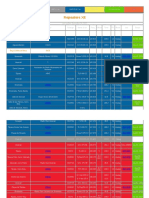
- Repeaters XE PDFDocument12 pagesRepeaters XE PDFenzzo molinariNo ratings yet
- Failure CountersDocument28 pagesFailure CountersБотирали АзибаевNo ratings yet
- Economic Globalization: Actors, Categories, and StagesDocument28 pagesEconomic Globalization: Actors, Categories, and StagesJoshua PunganNo ratings yet
- Giai Thich Ngu Phap Tieng Anh - Mai Lan Huong (Ban Dep)Document9 pagesGiai Thich Ngu Phap Tieng Anh - Mai Lan Huong (Ban Dep)Teddylove11No ratings yet
- Facebook Privacy FTC Complaint Docket No. C-4365Document19 pagesFacebook Privacy FTC Complaint Docket No. C-4365David SangerNo ratings yet
- 09 User Guide Xentry Diagnosis Kit 4 enDocument118 pages09 User Guide Xentry Diagnosis Kit 4 enDylan DY100% (2)
- Quiz 1Document6 pagesQuiz 1Eliza Mae Aquino100% (1)
- List of MeriendasDocument17 pagesList of MeriendasKristoffer OgalinoNo ratings yet
- Unit 3 Administrative AdjudicationDocument18 pagesUnit 3 Administrative AdjudicationkipkarNo ratings yet
- Whipping Cream PowderDocument2 pagesWhipping Cream PowderSALCON ConsultancyNo ratings yet
- Yale Film Analysis WebsiteDocument5 pagesYale Film Analysis WebsiteizmcnortonNo ratings yet
- Assessment - Lesson 1Document12 pagesAssessment - Lesson 1Charlynjoy AbañasNo ratings yet
- ĐỀ MINH HỌA 15-19Document25 pagesĐỀ MINH HỌA 15-19Trung Vũ ThànhNo ratings yet
- Reflecting Surfaces Discussion BibliographyDocument58 pagesReflecting Surfaces Discussion BibliographyAnanthanarayananNo ratings yet
- NUC BIOS Update Readme PDFDocument3 pagesNUC BIOS Update Readme PDFSuny Zany Anzha MayaNo ratings yet
- Oil Immersed TransformerDocument8 pagesOil Immersed TransformerAbdul JabbarNo ratings yet
- MR GMAT Combinatorics+Probability 6EDocument176 pagesMR GMAT Combinatorics+Probability 6EKsifounon KsifounouNo ratings yet
- MEPQ7202 Security OfficerDocument55 pagesMEPQ7202 Security OfficerSALMANNo ratings yet
- 11th House of IncomeDocument9 pages11th House of IncomePrashanth Rai0% (1)
- Rizal's First Return Home to the PhilippinesDocument52 pagesRizal's First Return Home to the PhilippinesMaria Mikaela MarcelinoNo ratings yet