You might also like
- IMMUNIZATION RECORD CERTIFICATEDocument2 pagesIMMUNIZATION RECORD CERTIFICATEanusdasari100% (10)
- IMMUNIZATION RECORD CERTIFICATEDocument2 pagesIMMUNIZATION RECORD CERTIFICATEanusdasari100% (10)
- Medical Record FormDocument4 pagesMedical Record FormДария КоваленкоNo ratings yet
- John Jay Immunization FormDocument3 pagesJohn Jay Immunization FormIsam BoukattayaNo ratings yet
- Communicablediseases 110227001506 Phpapp02 PDFDocument30 pagesCommunicablediseases 110227001506 Phpapp02 PDFCrystal Ann Monsale TadiamonNo ratings yet
- Infectious Disease Medical Behavioral Screens AmendedDocument6 pagesInfectious Disease Medical Behavioral Screens AmendedHengkyNo ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- PSW6 - PPHFDocument16 pagesPSW6 - PPHFanishthNo ratings yet
- Immunization Letter NB FORM RevisedDocument6 pagesImmunization Letter NB FORM RevisedUddhavendra Pal SinghNo ratings yet
- An Important FormDocument3 pagesAn Important FormRachel ColeNo ratings yet
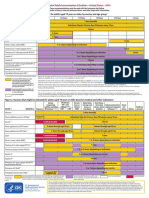
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Adult Immunization Schedule and RecommendationsDocument3 pagesAdult Immunization Schedule and RecommendationsdrmanojvimalNo ratings yet
- Immunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationDocument7 pagesImmunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationShubham TrivediNo ratings yet
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioNo ratings yet
- Pre Entrance Immunization FormDocument3 pagesPre Entrance Immunization FormsmithwesNo ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- Immunization Submission FormDocument3 pagesImmunization Submission Formdimpiu11No ratings yet
- Immreq15 16Document2 pagesImmreq15 16api-234991765No ratings yet
- Pre-Registration Nursing Information For Prospective StudentsDocument4 pagesPre-Registration Nursing Information For Prospective StudentsbthangarajNo ratings yet
- ScheduleDocument2 pagesScheduleapi-286634335No ratings yet
- Epi and Cold ChainDocument3 pagesEpi and Cold ChainShadrackNo ratings yet
- Adult Schedule 11x17Document2 pagesAdult Schedule 11x17lcmurilloNo ratings yet
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfNo ratings yet
- Health History and Immunization Form: University of Valley Forge - Health CenterDocument4 pagesHealth History and Immunization Form: University of Valley Forge - Health CenterBernard AmetepeNo ratings yet
- Recommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Document2 pagesRecommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Maja MudriNo ratings yet
- 01CIM 01 - Clinical Pathway Managing TB CasesDocument10 pages01CIM 01 - Clinical Pathway Managing TB Casesyin sNo ratings yet
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDocument24 pagesImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahNo ratings yet
- Immunization Requirement Form - UpdateDocument2 pagesImmunization Requirement Form - UpdateManojkumar ANo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- "Expanded Program On Immunization": Angeles University FoundationDocument12 pages"Expanded Program On Immunization": Angeles University FoundationJaillah Reigne CuraNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- Immunization History FormDocument1 pageImmunization History FormMohammad ShoiabNo ratings yet
- Standing Orders For Administering Tdap/Td To Adults: (Name of Practice or Clinic)Document1 pageStanding Orders For Administering Tdap/Td To Adults: (Name of Practice or Clinic)selvie87No ratings yet
- TUBERCULOSIS TB RISK ASSESSMENT FORM Created March 12 2018 1Document2 pagesTUBERCULOSIS TB RISK ASSESSMENT FORM Created March 12 2018 1Jimmy MountNo ratings yet
- FIU Immunization Documentation FormDocument2 pagesFIU Immunization Documentation FormMO MONo ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- Recommended Immunizations FS enDocument2 pagesRecommended Immunizations FS enirfanmajeed1987No ratings yet
- Reading VaccineImmunizationDocument13 pagesReading VaccineImmunizationelztly4694No ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- Health Information FormDocument13 pagesHealth Information FormArtero-Cavallaro PabloNo ratings yet
- ImmunizationDocument40 pagesImmunizationHilyaJae-heeNo ratings yet
- Preventing Illness and Living With Ill HealthDocument11 pagesPreventing Illness and Living With Ill HealthMonique MavronicolasNo ratings yet
- Running Head: Tdap Education and The Proper Administration 1Document4 pagesRunning Head: Tdap Education and The Proper Administration 1api-402463634No ratings yet
- St. Paul University PhilippinesDocument7 pagesSt. Paul University PhilippinesAngelica Mae Kidang RositeNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- GOVT.MODEL AYURVED COLLEGE STUDENT'S COMPILATION ON TYPHOID FEVER EPIDEMIOLOGY, SYMPTOMS AND CONTROLDocument16 pagesGOVT.MODEL AYURVED COLLEGE STUDENT'S COMPILATION ON TYPHOID FEVER EPIDEMIOLOGY, SYMPTOMS AND CONTROLArc MuNo ratings yet
- Population Growth Drives Disease SpreadDocument44 pagesPopulation Growth Drives Disease Spreadganesh8sundaresanNo ratings yet
- ImmunizationCertificate PDFDocument2 pagesImmunizationCertificate PDFAnonymous kq5iEDxxhrNo ratings yet
- Form PD1 Medical Examination ReportDocument9 pagesForm PD1 Medical Examination ReportSyazwi BaharuddinNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Vietnamese Student Health Exam GuidelinesDocument6 pagesVietnamese Student Health Exam GuidelinesKita 09No ratings yet
- Rutgers Immunization FormDocument3 pagesRutgers Immunization Formruhayl khanNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- Dalhousie Dentistry Immunization RequirementsDocument3 pagesDalhousie Dentistry Immunization Requirementsabhinav guptaNo ratings yet
- Immunization Requirement - Student Health Center - The University of UtahDocument2 pagesImmunization Requirement - Student Health Center - The University of Utahmithun916No ratings yet
- Your Name Institution/organization Meeting DateDocument42 pagesYour Name Institution/organization Meeting DateMochammad Fariz AmsalNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- EPIDocument7 pagesEPIheng_gutierrezNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Immunization RecordDocument2 pagesImmunization RecordNonofYaNo ratings yet
- Immunization RecordDocument1 pageImmunization RecordNonofYaNo ratings yet
- Immunization RecordDocument2 pagesImmunization RecordNonofYaNo ratings yet