You might also like
- Circumcision 2015 PDFDocument20 pagesCircumcision 2015 PDFlilikNo ratings yet
- Pedoman Up, Ip PDFDocument146 pagesPedoman Up, Ip PDFlilik100% (9)
- RoleOfFeminineHygiene - LactacydDocument1 pageRoleOfFeminineHygiene - LactacydlilikNo ratings yet
- Idi - 011115Document54 pagesIdi - 011115lilikNo ratings yet
- Grand City Manag Pe Presentation DR Nov 2015Document1 pageGrand City Manag Pe Presentation DR Nov 2015lilikNo ratings yet
- Circumcision 2015Document20 pagesCircumcision 2015lilikNo ratings yet
- Clinical Practice in Contraception-BUSDocument34 pagesClinical Practice in Contraception-BUSlilikNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Thiamine in Septic ShockDocument6 pagesThiamine in Septic ShockSrinivas PingaliNo ratings yet
- Patient AssesmentDocument1 pagePatient AssesmentVinceandHeidiNo ratings yet
- First Aid: Minor Cuts and ScratchesDocument2 pagesFirst Aid: Minor Cuts and ScratchesnorwalkreadymixNo ratings yet
- تجميعةDocument168 pagesتجميعةRn nadeenNo ratings yet
- Case Study Burn Injury - 11Document15 pagesCase Study Burn Injury - 11Evelyn MedinaNo ratings yet
- SBA questions on embryology, paediatrics, psychiatry and moreDocument3 pagesSBA questions on embryology, paediatrics, psychiatry and moreDamienNo ratings yet
- Index of Army Motion Pictures For PublicDocument61 pagesIndex of Army Motion Pictures For Publicssyd99No ratings yet
- Critical Care of The Burned PatientDocument222 pagesCritical Care of The Burned PatientYunita Manurung100% (1)
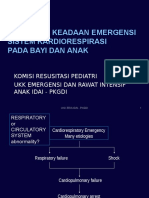
- Perawat DOKTER MengKegawatanAnak DadangDocument80 pagesPerawat DOKTER MengKegawatanAnak DadangLihinNo ratings yet
- Shock ManagementDocument26 pagesShock ManagementMuhammad Irfanuddin Bin IbrahimNo ratings yet
- Viva in Oral Surgery For Dental Students, 1E (2012) (PDF) (UnitedVRG)Document147 pagesViva in Oral Surgery For Dental Students, 1E (2012) (PDF) (UnitedVRG)Mubashir Sheriff79% (14)
- Obstructive Shock, From Diagnosis To TreatmentDocument10 pagesObstructive Shock, From Diagnosis To TreatmentJonathan PuenteNo ratings yet
- NURSING CARE ON CLIENTS WITH DIARRHEADocument30 pagesNURSING CARE ON CLIENTS WITH DIARRHEAyustiNo ratings yet
- Patofisiologi DiareDocument45 pagesPatofisiologi DiareAngela Kristiana Intan100% (1)
- Torres 7TH EditionDocument67 pagesTorres 7TH EditionDrexel DalaygonNo ratings yet
- Idiopathic Systemic Capillary Leak Syndrome - UpToDateDocument17 pagesIdiopathic Systemic Capillary Leak Syndrome - UpToDatenikos papamakariosNo ratings yet
- Sepsis 101: Colorado Hospital AssociationDocument27 pagesSepsis 101: Colorado Hospital Associationamal.fathullahNo ratings yet
- Hypovolemic Shock - StatPearls - NCBI BookshelfDocument1 pageHypovolemic Shock - StatPearls - NCBI BookshelfRoselyn VelascoNo ratings yet
- Kher 2017Document39 pagesKher 2017Evelyn LimNo ratings yet
- Mini VET GuideDocument186 pagesMini VET GuideemitibiNo ratings yet
- Cuthbertson 1942Document5 pagesCuthbertson 1942Saandy MirandaNo ratings yet
- Burns and Patient ManagementDocument85 pagesBurns and Patient ManagementDr Mohamed A. El Rouby94% (16)
- BURNDocument101 pagesBURNLexus Nosyel100% (1)
- Blood Lactate Levels in Sepsis in 8 QuestionsDocument5 pagesBlood Lactate Levels in Sepsis in 8 Questionsbenitez1228No ratings yet
- Medical Surgical Nursing Bullets (Nle & Nclex)Document105 pagesMedical Surgical Nursing Bullets (Nle & Nclex)Cuzii marieeNo ratings yet
- Sepsis - Eval and MGMTDocument62 pagesSepsis - Eval and MGMTDr Ankit SharmaNo ratings yet
- Pathology Assignment 2Document5 pagesPathology Assignment 2MahaaaNo ratings yet
- Medications Used in Code Blue EmergenciesDocument24 pagesMedications Used in Code Blue EmergenciesAhmed Ali Mohammed AlbashirNo ratings yet
- Buletin Mutiara Mac #2 IssueDocument48 pagesBuletin Mutiara Mac #2 IssueChan LilianNo ratings yet
- Rapid Pathology Pathology Textbook For Medical StudentsDocument89 pagesRapid Pathology Pathology Textbook For Medical Studentsyennqing100% (1)