You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Dinner Theater Business PlanDocument21 pagesDinner Theater Business PlanBhumika KariaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Installing Oracle Fail SafeDocument14 pagesInstalling Oracle Fail SafeSantiago ArgibayNo ratings yet
- Id or Class Are SimplyDocument5 pagesId or Class Are SimplyK CorNo ratings yet
- Toyota Auris Corolla 2007 2013 Electrical Wiring DiagramDocument22 pagesToyota Auris Corolla 2007 2013 Electrical Wiring Diagrampriscillasalas040195ori100% (125)
- Chip Expansion BriefDocument5 pagesChip Expansion Briefkirs0069No ratings yet
- Dependent Coverage Expansions Issue BriefDocument6 pagesDependent Coverage Expansions Issue Briefkirs0069No ratings yet
- LouisianaCaseStudy BriefDocument5 pagesLouisianaCaseStudy Briefkirs0069No ratings yet
- Vermont Comprehensive ReformDocument6 pagesVermont Comprehensive Reformkirs0069No ratings yet
- Sci Brief FinalDocument12 pagesSci Brief Finalkirs0069No ratings yet
- SHARE Report Cousineau FinalDocument7 pagesSHARE Report Cousineau Finalkirs0069No ratings yet
- IncomeEligibilityUnderACA FINAL v2Document6 pagesIncomeEligibilityUnderACA FINAL v2kirs0069No ratings yet
- StateProgramsReform REPORTDocument59 pagesStateProgramsReform REPORTkirs0069No ratings yet
- EligibilityChangesStateIssues Brief1Document6 pagesEligibilityChangesStateIssues Brief1kirs0069No ratings yet
- ComparingFedSurveys 2008Document6 pagesComparingFedSurveys 2008kirs0069No ratings yet
- LessonsFromImplementation KidsFirst October2012Document4 pagesLessonsFromImplementation KidsFirst October2012kirs0069No ratings yet
- StateProgramsUnderReform BriefDocument8 pagesStateProgramsUnderReform Briefkirs0069No ratings yet
- ComparingFedSurveys 2009Document7 pagesComparingFedSurveys 2009kirs0069No ratings yet
- Comparing Federal Government Surveys That Count The UninsuredDocument9 pagesComparing Federal Government Surveys That Count The Uninsuredkirs0069No ratings yet
- RWJF CompareSurveysIB Aug2007Document7 pagesRWJF CompareSurveysIB Aug2007kirs0069No ratings yet
- Www.sefindia.orgDocument372 pagesWww.sefindia.orgRahul KolateNo ratings yet
- 10.isca RJCS 2015 106Document5 pages10.isca RJCS 2015 106Touhid IslamNo ratings yet
- BCCA Semester New Syllabus Direction 2016-17 PDFDocument76 pagesBCCA Semester New Syllabus Direction 2016-17 PDFChetana Gorakh100% (1)
- Forecasting and Demand Management PDFDocument39 pagesForecasting and Demand Management PDFKazi Ajwad AhmedNo ratings yet
- AbDocument8 pagesAbSehar BanoNo ratings yet
- Katalog Bonnier BooksDocument45 pagesKatalog Bonnier BooksghitahirataNo ratings yet
- Objectives in DraftingDocument1 pageObjectives in Draftingshannejanoras03No ratings yet
- Sworn Statement of Assets, Liabilities and Net WorthDocument2 pagesSworn Statement of Assets, Liabilities and Net WorthFaidah Palawan AlawiNo ratings yet
- Application For Leave - EODocument1 pageApplication For Leave - EOcomelec carmenNo ratings yet
- HOVAL Dati Tecnici Caldaie IngleseDocument57 pagesHOVAL Dati Tecnici Caldaie Ingleseosama alabsiNo ratings yet
- Manual Teclado GK - 340Document24 pagesManual Teclado GK - 340gciamissNo ratings yet
- SS 671Document9 pagesSS 671OwNo ratings yet
- Microsoft Software License Terms Microsoft Windows Media Player Html5 Extension For ChromeDocument2 pagesMicrosoft Software License Terms Microsoft Windows Media Player Html5 Extension For ChromeOmar PiñaNo ratings yet
- Manual de Parts ES16D6Document36 pagesManual de Parts ES16D6Eduardo CortezNo ratings yet
- Buffett Wisdom On CorrectionsDocument2 pagesBuffett Wisdom On CorrectionsChrisNo ratings yet
- Unit 1 Notes (Tabulation)Document5 pagesUnit 1 Notes (Tabulation)RekhaNo ratings yet
- EquisetopsidaDocument4 pagesEquisetopsidax456456456xNo ratings yet
- Dorma 2012 Price ListDocument284 pagesDorma 2012 Price ListSecurity Lock DistributorsNo ratings yet
- Class Assignment 2Document3 pagesClass Assignment 2fathiahNo ratings yet
- A 150.xx Service Black/ITU Cartridge Motor Error On A Lexmark C54x and X54x Series PrinterDocument4 pagesA 150.xx Service Black/ITU Cartridge Motor Error On A Lexmark C54x and X54x Series Printerahmed salemNo ratings yet
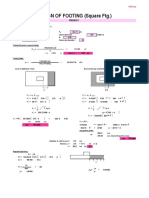
- Design of Footing (Square FTG.) : M Say, L 3.75Document2 pagesDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNo ratings yet
- Food Truck Ordinance LetterDocument7 pagesFood Truck Ordinance LetterThe Daily News JournalNo ratings yet
- STAAD Seismic AnalysisDocument5 pagesSTAAD Seismic AnalysismabuhamdNo ratings yet
- AKROLEN® PP ICF 30 AM Black (8344) - Akro-PlasticDocument3 pagesAKROLEN® PP ICF 30 AM Black (8344) - Akro-PlasticalkhalidibaiderNo ratings yet
- VMC Ballscrew 32mm Horizontal Plane ReplacementDocument11 pagesVMC Ballscrew 32mm Horizontal Plane ReplacementMarlon GeronimoNo ratings yet
- Addendum No.1: Indianapolis Metropolitan Airport T-Hangar Taxilane Rehabilitation IAA Project No. M-12-032Document22 pagesAddendum No.1: Indianapolis Metropolitan Airport T-Hangar Taxilane Rehabilitation IAA Project No. M-12-032stretch317No ratings yet